TABLE OF CONTENTS
Chabertia ovina (Large-Mouthed Bowel Worm): Morphology, Life Cycle, Clinical Signs, Diagnosis & Treatment
Chabertia ovina, commonly known as the large-mouthed bowel worm, is a parasitic nematode of sheep, goats, cattle, and other ruminants. It primarily inhabits the colon and is distributed worldwide. Although infections are often subclinical, heavy worm burdens can cause parasitic gastroenteritis, diarrhea, weight loss, anemia, and reduced productivity, particularly in sheep.
This article provides a comprehensive overview of Chabertia ovina, including its taxonomical classification, morphology, life cycle, pathogenesis, clinical signs, diagnosis, and treatment.
The infective stage is the third-stage larva (L3), which is acquired through the ingestion of contaminated herbage during grazing.
Parasite Overview
- Common Name: Large-mouthed bowel worm
- Host: Sheep, goats, cattle, and other ruminants
- Location: Colon
- Distribution: Worldwide
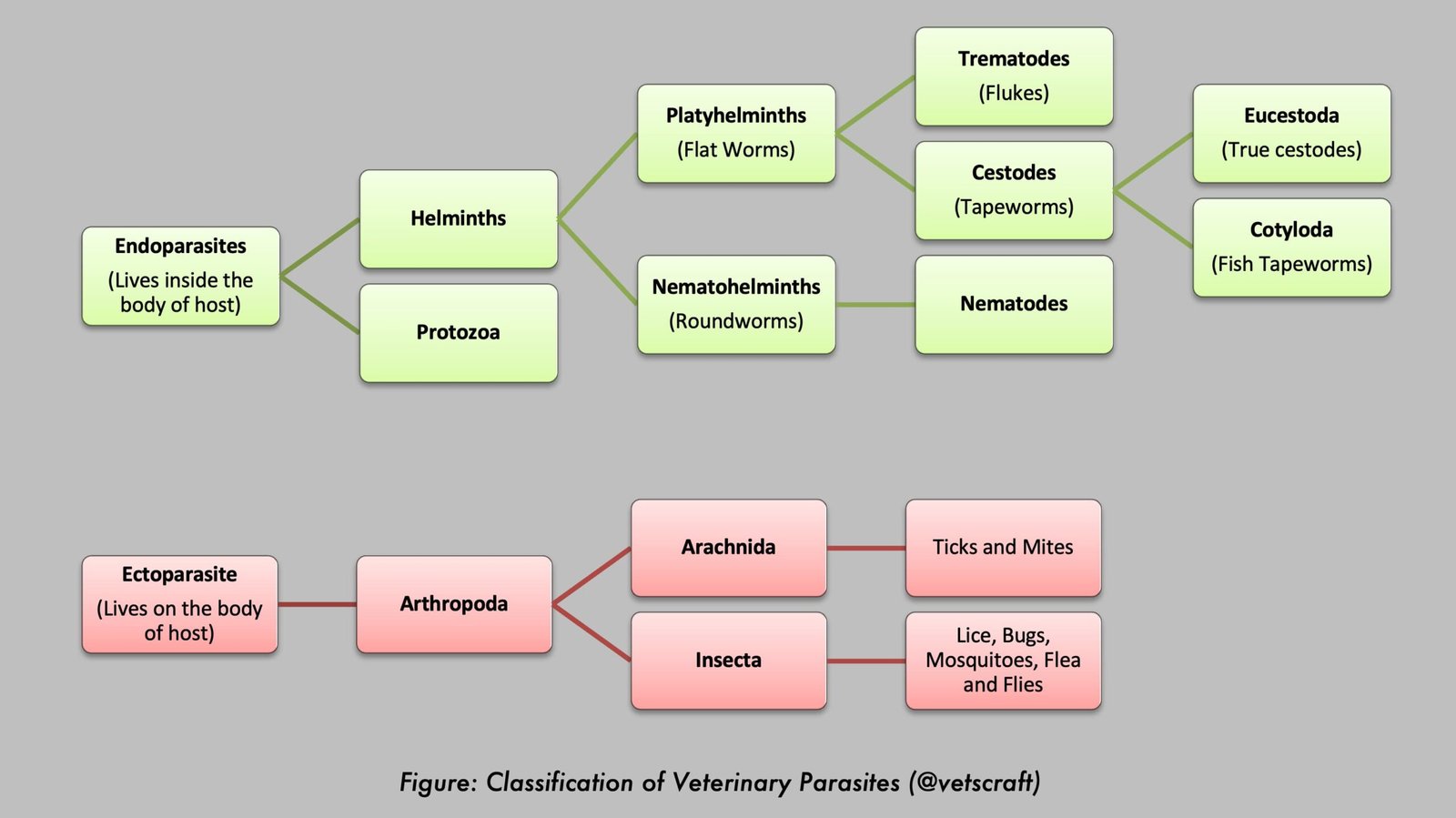
Taxonomical Classification
- Kingdom: Animalia
- Phylum: Nematoda
- Class: Chromadorea
- Order: Strongylida
- Family: Chabertiidae (formerly Trichonematidae)
- Genus: Chabertia
- Species: Chabertia ovina
- Common Name: Large-mouthed bowel worm
Morphology
- 1–2 cm in length.
- The anterior end is curved slightly ventrally.
- The large buccal capsule opens anteroventrally and is bell-shaped.
- The oral aperture is surrounded by a double row of small cuticular elements, resembling leaf crowns (papillae).
- A shallow ventral cervical groove is present, and anterior to it is a slightly inflated cephalic vesicle.
- No teeth.
- Eggs are typical strongyle eggs.
Life Cycle
- Direct life cycle; mode of infection: per os.
- Infective stage: L3; prepatent period: 49 days.
The eggs are passed in the feces and hatch on the ground, releasing the L1, which molts to the L2 and then to the infective L3. The host becomes infected by ingesting the larvae with herbage.
During the parasitic phase, the L3 enter the mucosa of the small intestine and occasionally that of the cecum and colon. After a week, they molt, and the L4 emerge onto the mucosal surface and migrate to congregate in the cecum, where development to the L5 is completed about 25 days after infection.
The young adults then migrate to the colon. There is no migratory phase in the body. The prepatent period is about 6–7 weeks.
Pathogenesis
Chabertia ovina is present, usually in low numbers, in the majority of sheep and goats. It contributes to the syndrome of parasitic gastroenteritis and only causes clinical disease on its own when present in sufficient numbers.
The major pathogenic effect is caused by the L5 and mature adults. They attach firmly to the mucosa of the colon via their buccal capsules and feed by ingesting large plugs of tissue, resulting in local hemorrhage and protein loss through the damaged mucosa.
They accidentally ingest blood while feeding. A burden of around 300 worms is considered pathogenic, and in severe outbreaks, the effects become evident during the late prepatent period. The wall of the colon becomes edematous, congested, and thickened, with small hemorrhages at the sites of worm attachment.
At necropsy, petechial punctiform hemorrhages are present in the colonic mucosa due to immature worms. Immature and adult worms are found in the lumen of the intestine. The mucosa is swollen, edematous, congested, and covered with mucus.
Clinical Signs
Moderate infections are usually asymptomatic. In severe infections, diarrhea, which may contain blood and mucus and in which worms may be found, is the most common clinical sign.
Sheep become anemic and hypoalbuminemic and may suffer severe weight loss. Chabertia infections may be responsible for a specific reduction in wool growth in sheep.
Diagnosis
Since much of the pathogenic effect occurs during the prepatent period, the fecal egg count may be very low. However, during the diarrheic phase, the worms may be expelled and are easily recognized.
At necropsy, diagnosis is generally based on the lesions, since the worm burden may be negligible following the expulsion of worms in the feces, although in some cases worms may be observed attached to the mucosa of the colon.
Treatment
Anthelmintic therapy with broad-spectrum anthelmintics (benzimidazoles, levamisole, and avermectins/milbemycins) is highly effective.