TABLE OF CONTENTS
Thelazia (Eye Worm): Morphology, Life Cycle, Pathogenesis, Diagnosis & Treatment
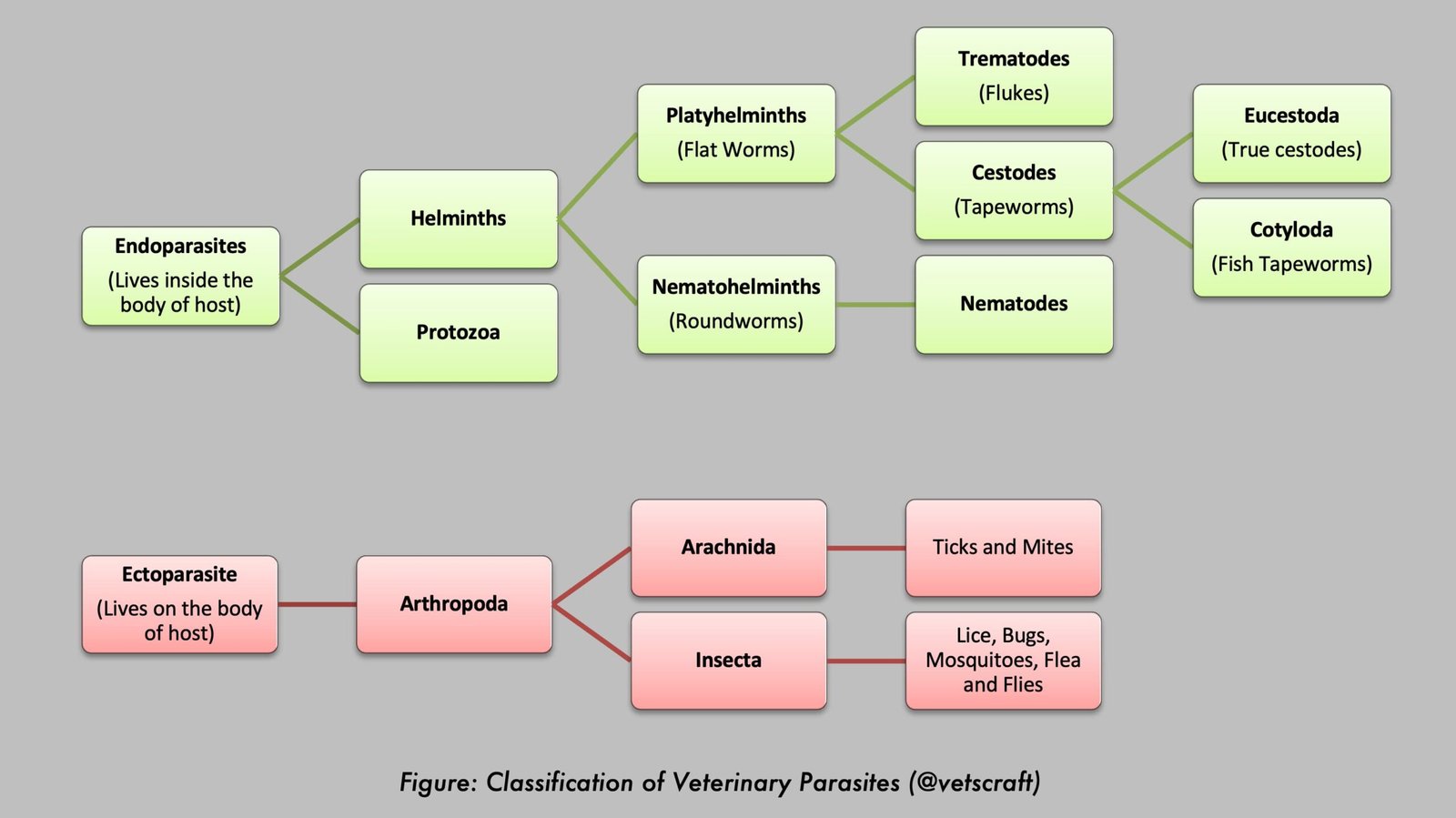
Thelazia, commonly known as the eye worm, is a genus of spirurid nematodes that parasitize the eyes and associated tissues of domestic and wild animals. These parasites inhabit the conjunctival sac, lacrimal ducts, and nictitating membrane, where they may cause conjunctivitis, keratitis, excessive lacrimation, and other ocular disorders.
Transmission occurs through secretophagous flies that act as intermediate hosts. Some Thelazia species are also zoonotic and can infect humans. This article covers the taxonomy, morphology, life cycle, pathogenesis, clinical signs, diagnosis, and treatment of Thelazia infections in animals.
The following Thelazia species are commonly encountered in animals:
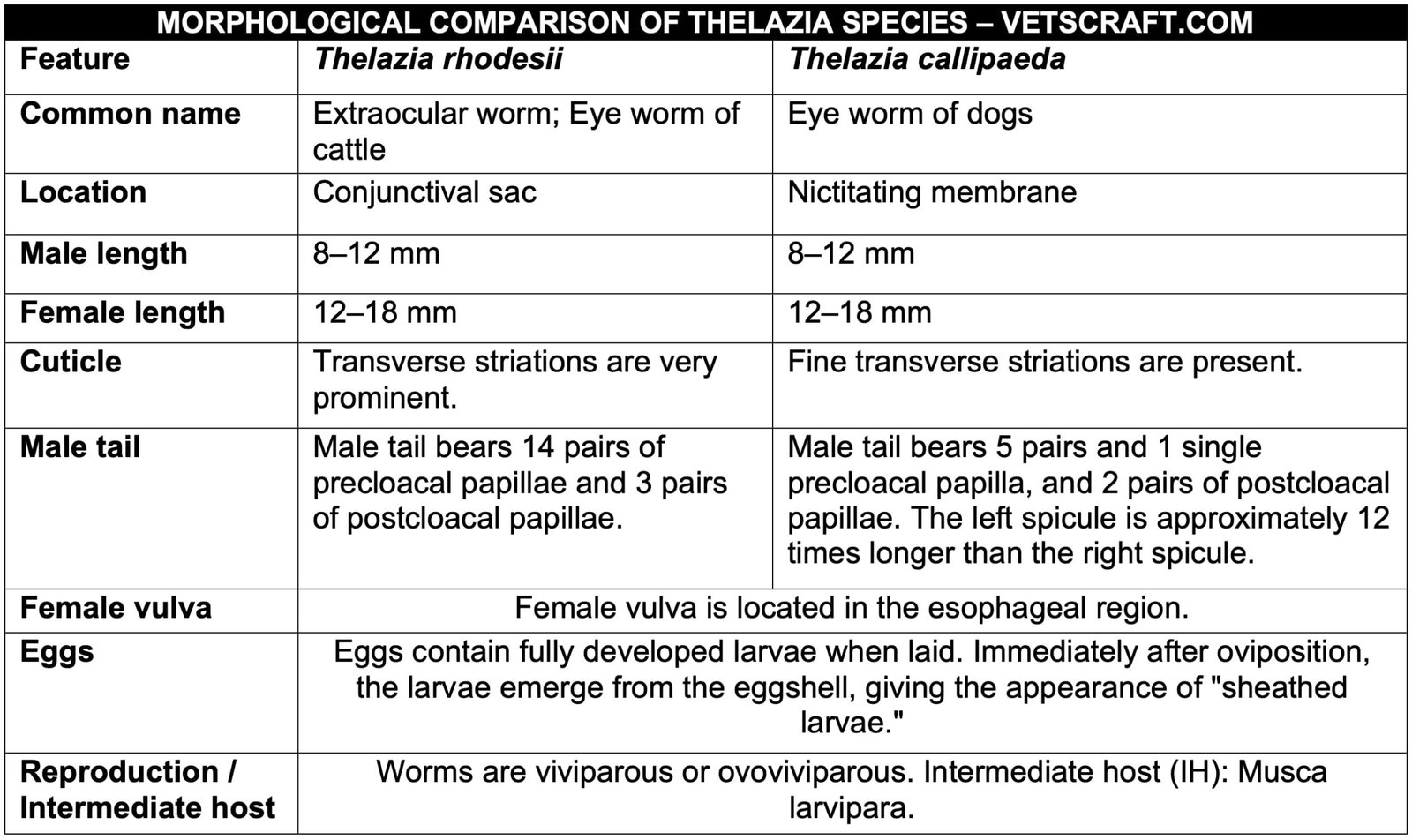
- Thelazia rhodesii: Eye worm of cattle
- Thelazia callipaeda: Eye worm of dogs
- Thelazia lacrymalis: Eye worm of horses
Taxonomical Classification of Thelazia (Eye Worm)
- Kingdom: Animalia
- Phylum: Nematoda
- Class: Secernentea (Phasmidia)
- Order: Spirurida
- Family: Thelaziidae
- Genus: Thelazia
- Important Species: Thelazia callipaeda, Thelazia californiensis, Thelazia gulosa, Thelazia rhodesii, Thelazia lacrymalis
- Common Name: Eye Worm
Morphology
Life Cycle
Adult flies ingest first-stage larvae (L1) while feeding on the ocular secretions of the definitive host (D/H). Following ingestion, the L1 larvae reach the gut of the fly and then penetrate the ovarian follicles, where they molt into L2 and subsequently into L3.
The infective L3 larvae migrate to the mouthparts of the fly and are transmitted to susceptible animals when the infected fly feeds.
Transmission is seasonal and generally does not occur during the winter months. Humans may also serve as accidental hosts when infected flies feed on tears or lacrimal secretions.
Pathogenesis
Adult worms are found beneath and within the nictitating membrane, lacrimal glands, nasolacrimal ducts, and on the surface of the conjunctival sac. Generally, adult parasites are not pathogenic in adult animals. However, in some cases, they may cause keratitis and ophthalmia.
Clinical Signs
- Lesions may be present in one or both eyes.
- Initially, there is mild conjunctivitis, followed by congestion of the conjunctiva and cornea.
- In severe cases, the cornea becomes cloudy, with marked lacrimation. The affected eye becomes markedly swollen and is covered with exudate and pus.
- If the condition is not treated properly, progressive keratitis and corneal ulceration may lead to protrusion of the anterior chamber of the eye.
- T. callipaeda and T. alfortensis infections in animal and human hosts may be asymptomatic; however, they frequently cause watery eyes (epiphora), conjunctivitis, corneal opacity, or corneal ulcers (ulcerative keratitis).
- Infested humans may also report a foreign body sensation (the feeling that something is in the eye). Follicular hypertrophy of the conjunctiva, excessive lacrimation, and hypersensitivity to light may also be observed.
- The condition may become more severe if a secondary bacterial infection develops.
Diagnosis
- Demonstration of the adult parasite under local anesthesia.
- Examination of lacrimal secretions for the presence of eggs or first-stage larvae (L1).
Management, Therapy, and Treatment
Remove the worms using fine forceps under local anesthesia. Pharmacological management includes irrigation with Lugol’s iodine or 2–3% boric acid immediately after worm removal or for parasites located within the lacrimal ducts that cannot be removed manually.
- Methyridine: 20 mL via the subconjunctival route
- Tetramisole: 15 mg/kg body weight
- Levamisole: 5 mg/kg body weight orally (it is excreted in lacrimal gland secretions) or 2 mL injected into the conjunctival sac.