TABLE OF CONTENTS
Dirofilaria immitis & Dirofilaria repens: Morphology, Life Cycle, Pathogenesis, Diagnosis & Treatment
Dirofilaria immitis and Dirofilaria repens are filarial nematodes of major veterinary and zoonotic importance. D. immitis, commonly known as the canine heartworm, primarily inhabits the pulmonary arteries and right ventricle of dogs, whereas D. repens is found in the subcutaneous connective tissues. Both species are transmitted by mosquitoes and can infect a wide range of mammalian hosts, including dogs, cats, wild carnivores, humans, and horses.
Heartworm disease caused by D. immitis is a serious cardiopulmonary disorder that can lead to pulmonary hypertension, congestive heart failure, and even death if left untreated. In contrast, D. repens typically causes subcutaneous infections but is also recognized as an emerging zoonotic parasite in many regions.
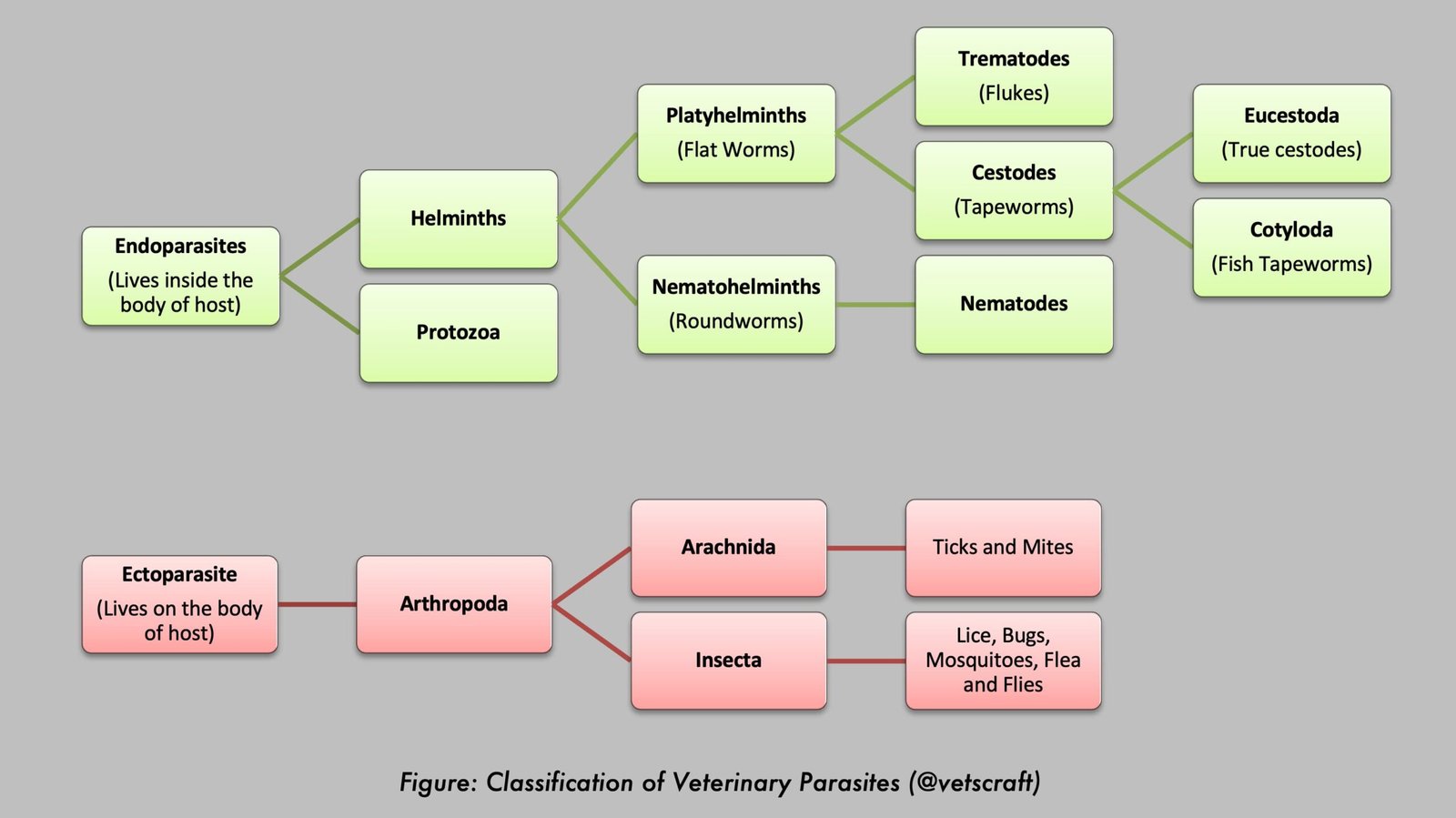
Parasite Overview
- Species: Dirofilaria immitis (Found in the right ventricle and pulmonary artery), Dirofilaria repens (Found in the subcutaneous connective tissues)
- Intermediate Hosts: Mosquitoes (Culex, Aedes, and Anopheles spp.)
- Predilection Site: Dirofilaria immitis (heartworm of dogs) lives in the right ventricle and pulmonary artery.
- Common Name: Filarial worms (heartworm and subcutaneous filarial worms)
Taxonomical Classification of Dirofilaria
- Kingdom: Animalia
- Phylum: Nematoda
- Class: Chromadorea
- Order: Spirurida
- Superfamily: Filarioidea
- Family: Onchocercidae
- Genus: Dirofilaria
- Important Species: Dirofilaria immitis, Dirofilaria repens
Morphology
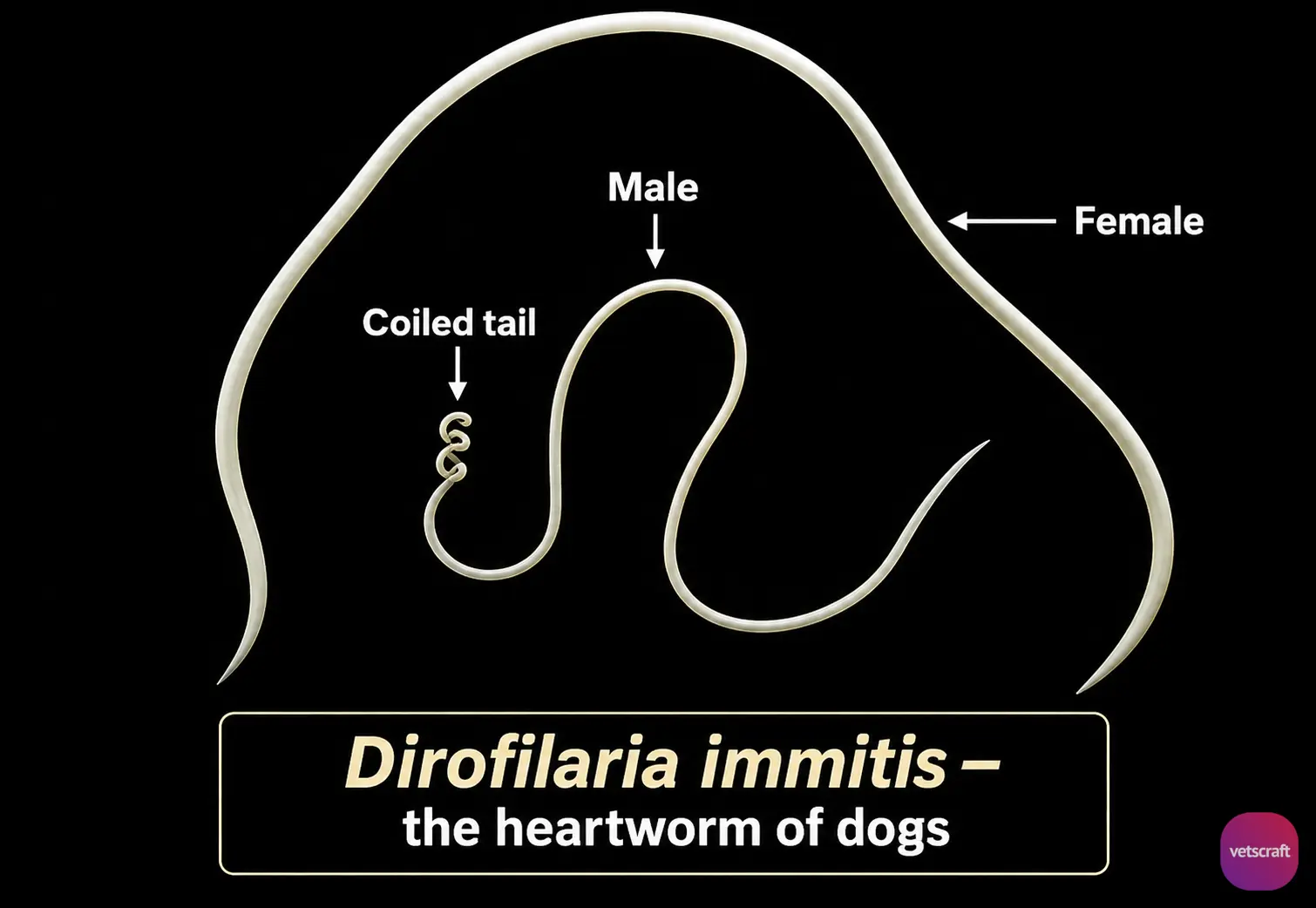
- Worms are long, thin, and white in color.
- Male: 12–16 cm; Female: 25–30 cm. The mouth is very small, and lips are absent.
- The esophagus has an anterior muscular and a posterior glandular portion.
- The posterior end of the male is spirally coiled, and the tail has lateral alae.
- The spicules are unequal; the left spicule is long and pointed, whereas the right is blunt.
- They are ovoviviparous.
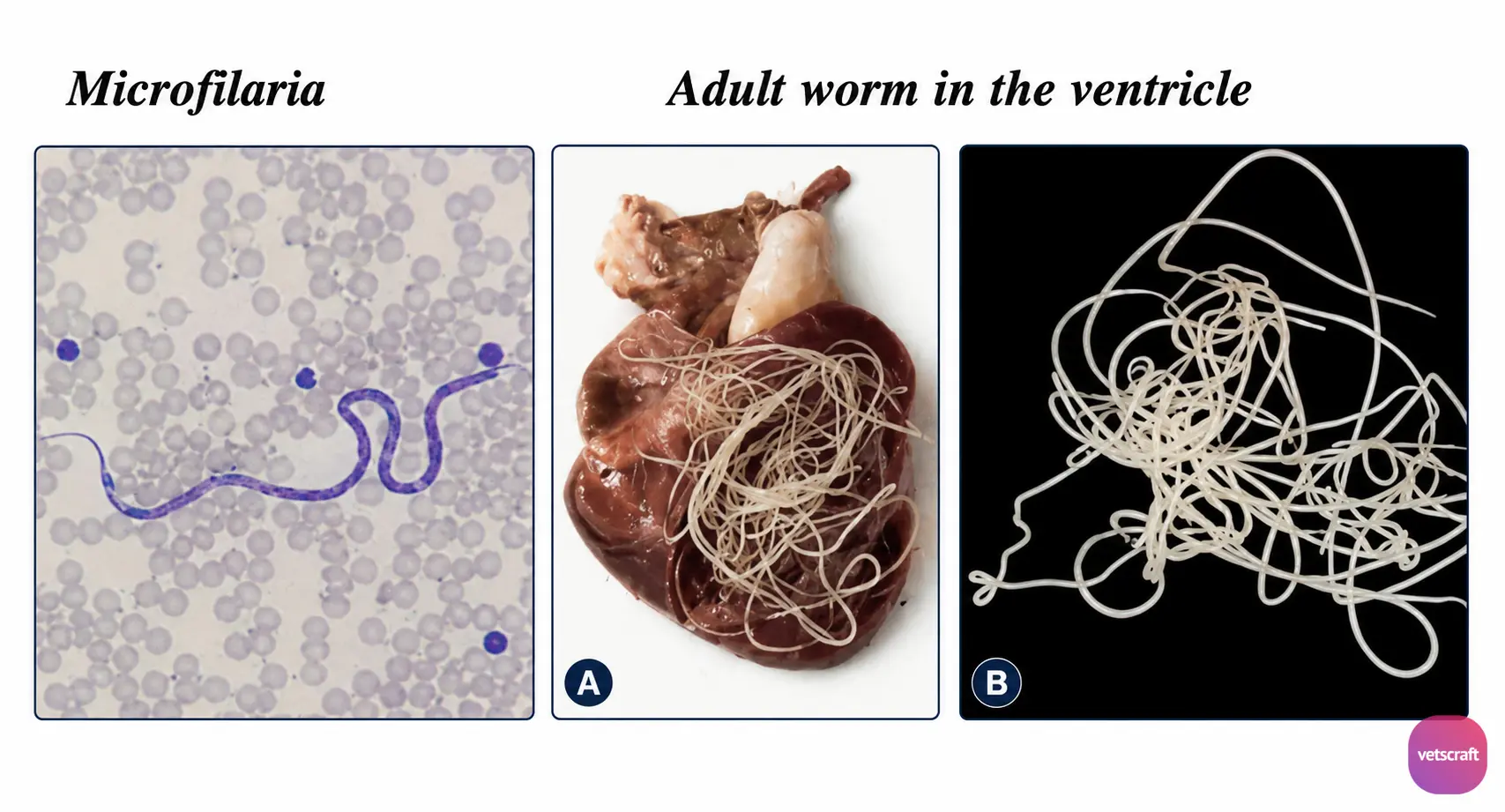
- The larva of filarids is known as the microfilaria, which is found in the blood of the host at all times.
Life Cycle
L1 (first-stage larvae) circulate in the bloodstream and infect mosquitoes. Mature female heartworms are ovoviviparous and release unsheathed, motile, vermiform embryos into the host’s bloodstream.
Adult mosquitoes ingest the microfilariae along with a blood meal while feeding on the definitive host. The ingested microfilariae are first found in the mosquito’s stomach and then migrate to the Malpighian tubules within 48 hours after ingestion, where further development occurs.
In about 4 days, they develop into a sausage form, a non-motile larva that is shorter and thicker (L2 stage). The sausage form becomes an elongated sausage form in about 9 days. It feeds on the cells of the Malpighian tubules and enters the hemocoel. From there, it migrates through the thorax and reaches the mouthparts, where it becomes the infective stage.
Dogs become infected when infected mosquitoes feed on them. Juvenile worms migrate through the tissues and reach the pulmonary arteries approximately 70–90 days after infection, where they continue to develop.
Approximately 6–7 months after infection, the worms reach sexual maturity, and adult females release microfilariae into the bloodstream, where they may survive for up to 2–7 years.
Pathogenesis
Mild infection causes no clinical signs, whereas heavy infection causes circulatory distress due to mechanical interference and progressive endarteritis.
The presence of a large number of worms in the heart interferes with the function of the cardiac valves. The right side of the heart becomes dilated and hypertrophied, leading to congestion, liver cirrhosis, and ascites.
Initially, ventricular hypertrophy develops, followed by cardiac dilatation. Edema of the lungs, kidneys, and liver, along with portal hypertension, intestinal congestion, and hydrothorax, may occur. Heartworm disease primarily causes pulmonary circulatory disturbances, leading to pulmonary hypertension due to narrowing of the peripheral pulmonary arteries.
Compensatory hypertrophy of the right ventricle results in congestive heart failure, liver failure syndrome, ascites, and peripheral edema.
Heartworm Disease in Cats
Clinically affected cats may present with a wide range of clinical signs, such as chronic coughing, labored breathing, and vomiting. Some infected cats die suddenly without any premonitory signs (acute death syndrome) due to acute pulmonary arterial infarction. However, many cats are subclinically infected, and the infection tends to be self-limiting.
Clinical Signs
Deep, soft cough, hemoptysis, reduced stamina, rapid breathing, a heart murmur, collapse, and dark brown urine containing hemoglobin and bilirubin. Anorexia and anemia may also be observed.
Diagnosis
Diagnosis is based on clinical signs and blood smear examination for the demonstration of microfilariae.
- Filter Method: One mL of blood in an anticoagulant is lysed with 0.1% Na2CO3. The blood is passed through a filter containing methylene blue and stained with methylene blue.
- Knott’s Method: One mL of blood is mixed with 9 mL of 2% formalin and centrifuged for 5 minutes. The sediment is then stained with one drop of a 1:1000 methylene blue solution.
- Thoracic radiography, ECG, serological tests, and immunodiagnostic tests such as ELISA and IFAT.
Treatment (Against Microfilariae)
- DEC: 5.5 mg/kg body weight for 2 months.
- Dithiazanine: 2 mg/0.45 kg body weight for 7 days.
- Levamisole: 10 mg/kg body weight for 15–20 days.
- Ivermectin: 0.05–0.1 mg/kg body weight, SC injection.
Treatment for Adult Worms
Melarsomine dihydrochloride at 2.5 mg/kg deep IM and thiacetarsamide at 0.1 mL/0.45 kg body weight IV can produce good results.
Prophylaxis
Treat affected dogs and adopt mosquito control measures. Drugs such as DEC (5.5 mg/kg body weight for 2 months) and mebendazole (80 mg/kg body weight for 30 days) can be administered.