TABLE OF CONTENTS
Intestinal Amoebiasis (Amoebic Dysentery): Symptoms, Diagnosis, Treatment & Prevention
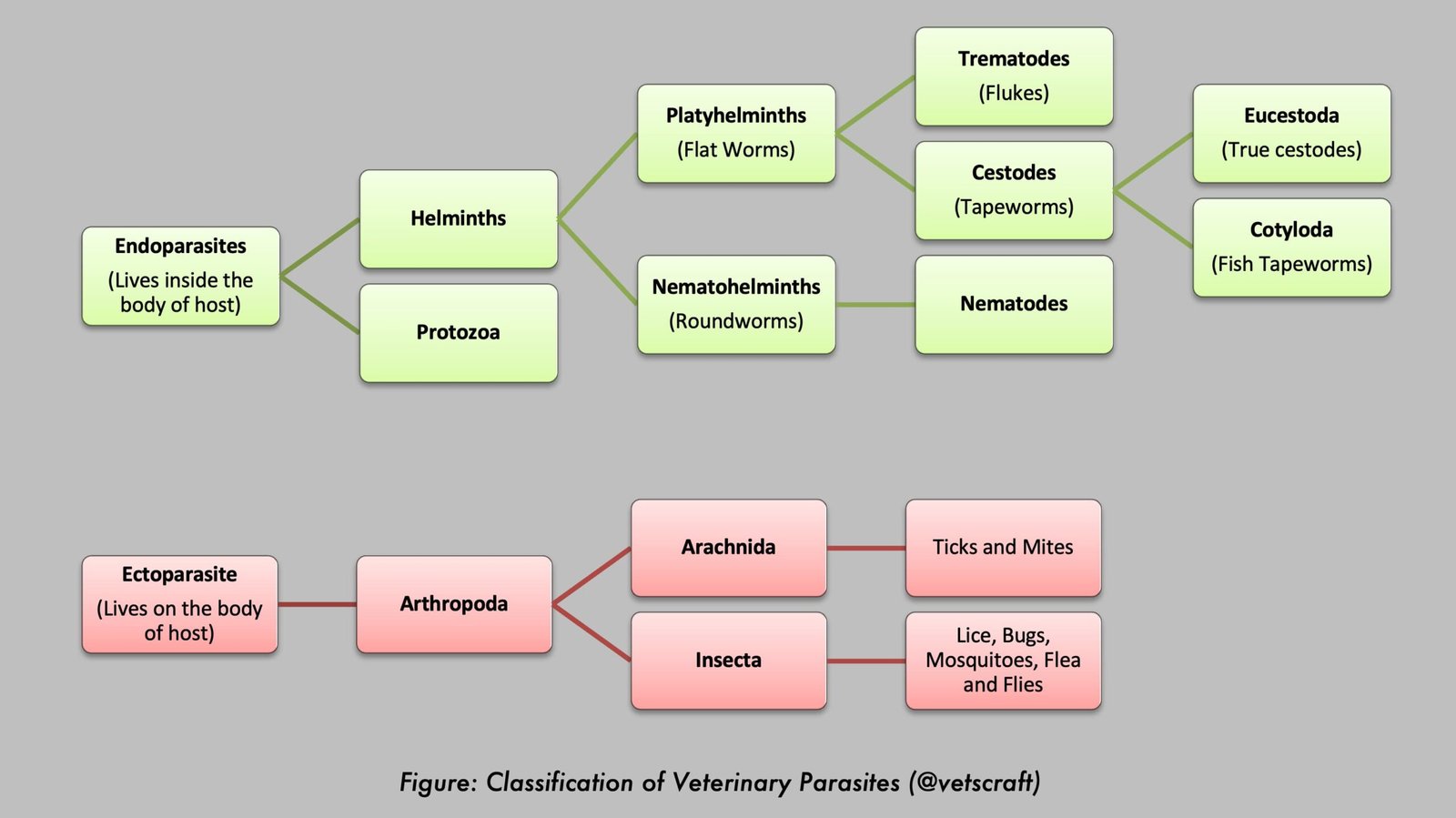
Intestinal amoebiasis, also known as amoebic dysentery, is an infectious disease caused by the protozoan parasite Entamoeba histolytica. It primarily affects the large intestine, where the invading trophozoites destroy the intestinal mucosa, resulting in ulcer formation, dysentery, and colitis. In severe cases, the parasite may spread beyond the intestine to organs such as the liver, lungs, and brain, leading to extraintestinal amoebiasis.
The disease is transmitted through the fecal–oral route by ingestion of mature cysts in contaminated food or water. Although many infected individuals remain asymptomatic, others may develop abdominal pain, diarrhea, bloody stools, and tenesmus. Diagnosis is based on the demonstration of cysts or trophozoites in fecal samples, supported by serological and imaging techniques when necessary. Treatment primarily involves nitroimidazole drugs, while effective prevention depends on proper sanitation, safe drinking water, food hygiene, and personal hygiene practices.
Pathology of Intestinal Amoebiasis
The large trophozoites penetrate the mucosa of the large intestine by lysing the epithelium, leading to necrosis and ulcer formation. Lysis of epithelial cells is brought about by proteolytic enzymes such as pepsin and trypsin. Following invasion of the epithelium, the trophozoites multiply and form small colonies.
Thereafter, they penetrate deeper tissues and reach the submucosa, where they cause extensive tissue destruction and spread laterally. This leads to weakening of the mucous membrane overlying the lesions and the formation of a flask-shaped ulcer, which has a narrow canal or neck leading to the lumen of the bowel and a dilated distal portion in the submucosa.
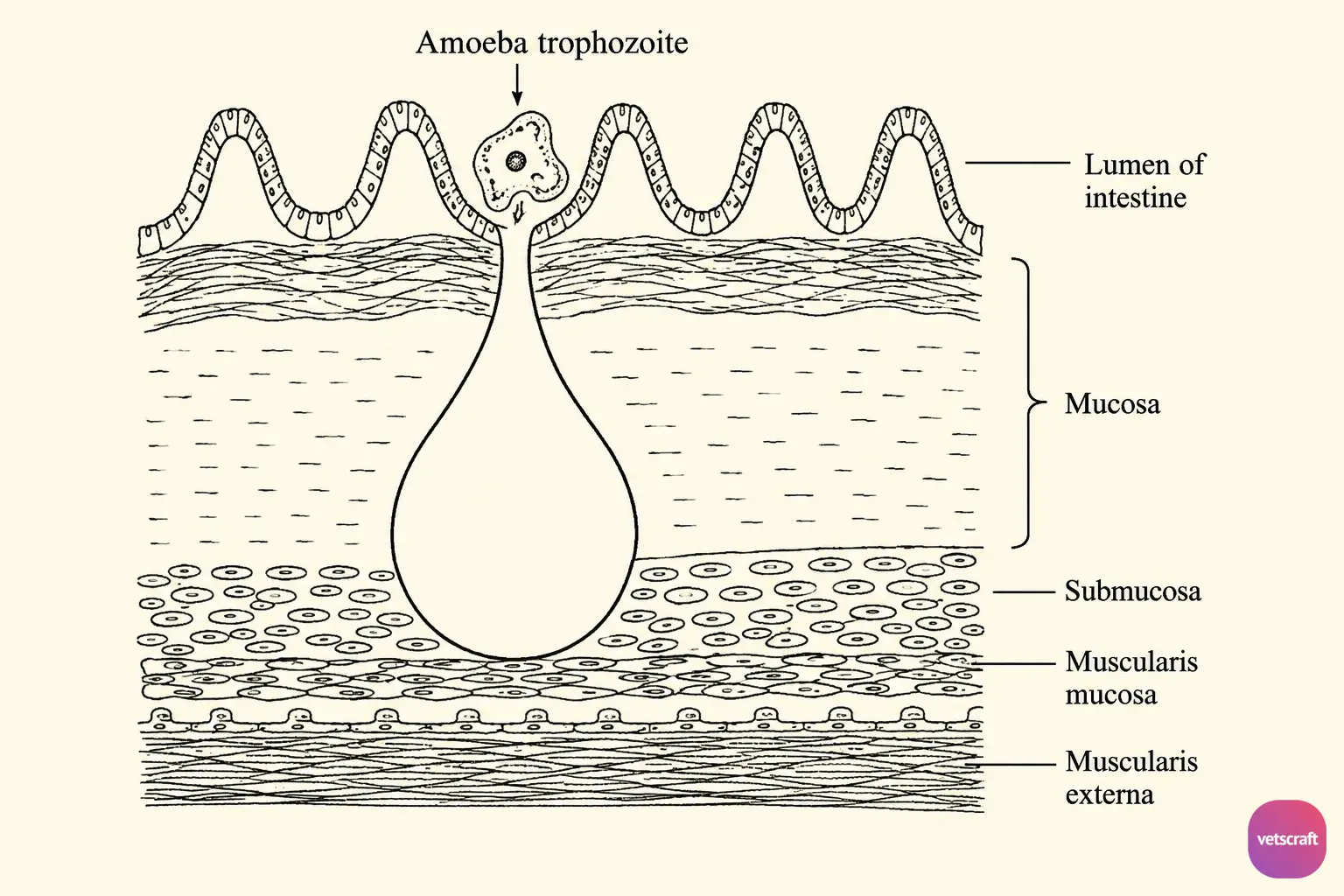
Initially, the lesions are seen in the caecum and ascending colon, showing little cellular reaction or bacterial invasion. If the lesions remain confined to the muscularis mucosa, the repair process may occur, followed by spontaneous elimination of the organisms.
In other cases, if the amoebae penetrate deeper layers of the intestinal wall, bacterial invasion occurs along with associated hyperaemia, inflammation, and neutrophilic infiltration.
Amoebae are chiefly found at the periphery of the ulcer and gradually penetrate the adjacent healthy tissue, leaving the ulcer cavity filled with necrotic tissue. Sometimes, the lesion perforates the intestinal wall, resulting in peritonitis.
Occasionally, the amoebae may stimulate granuloma formation in the large intestine, known as an amoeboma, which contains purulent fluid and trophozoites. This granulomatous growth may obstruct the intestinal lumen.
Extraintestinal Amoebiasis: Sometimes, the amoebae are carried through the blood or lymphatic system to various organs such as the liver, lungs, and brain, where they cause abscess formation.
Pathogenesis in Domestic Animals
Animals acquire the infection from humans through direct contact during handling and feeding. In dogs and kittens, E. histolytica does not produce cysts. In dogs, lesions are mainly observed in the large intestine and may also occur in the liver, lungs, kidneys, and spleen. Affected animals develop haemorrhagic enteritis, dysentery, colic, and stools that are mucus-coated, blood-tinged, and foul-smelling. The intestinal mucosa becomes inflamed and ulcerated.
Clinical Signs and Symptoms
The incubation period is 2–5 days, and clinical signs vary considerably between cases. They depend on the host’s natural or acquired resistance, the infecting strain, and the individual’s physical condition.
Some patients may tolerate intestinal amoebiasis for years without showing signs of colitis, although they continue to pass cysts in the faeces. They may also develop extraintestinal lesions later.
Intestinal amoebiasis develops gradually with intermittent diarrhoea, abdominal cramps, vomiting, general malaise, and weight loss.
Affected patients experience pain throughout the abdomen and fulminant dysentery occurring 4–6 times daily with tenesmus. The faeces are foul-smelling, dark red, and mixed with blood and mucus.
- In hepatic amoebiasis, there is enlargement of the liver, intermittent fever, and pain in the upper right abdomen.
- In pulmonary amoebiasis, there may be pain in the lower right region of the chest and cough. If abscesses rupture, grayish-brown material may be expectorated, and dyspnoea may be observed.
Diagnosis
- Clinical signs.
- Demonstration of Cysts: Cysts are usually passed in well-formed faeces. During examination of fresh faeces, a drop of iodine in 1% potassium iodide is added to facilitate recognition of cysts. Cysts can be concentrated using a zinc sulphate flotation solution; however, salt and sugar solutions should not be used as they cause distortion.
- Demonstration of Trophozoites: Trophozoites may also be passed in the faeces during acute diarrhoeic cases. Therefore, diarrhoeic faeces are mixed with normal saline and examined microscopically by direct wet mount for the demonstration of trophozoites.
- Specific diagnosis can be made by examining permanent faecal smears stained with iron hematoxylin after fixation in Schaudinn’s solution.
- Radiographic diagnosis can be employed for extraintestinal amoebiasis.
- Serological tests: IHA, indirect immunofluorescence, and CIEP.
- Isolation of Organisms: Suspected fresh material can be inoculated into Balamuth’s medium.
- Animal inoculation.
Treatment
Treatment of intestinal amoebiasis depends on the severity of infection and whether extraintestinal involvement is present. Metronidazole remains the drug of choice for invasive amoebiasis, followed by luminal amoebicides when indicated.
- Dehydroemetine: 30–60 mg SC or 25 mg orally three times daily for 10 days.
- Chloroquine: 300 mg orally three times daily for 2 days.
- Metronidazole: 400 mg three times daily for 5–10 days (drug of choice).
- Tinidazole: 2 g initially, followed by 500 mg twice daily for 5 days.
- Secnidazole: 2 g initially, followed by 300 mg three times daily for 5 days.
- Ornidazole: 1.5 g initially, followed by 500 mg daily for 10 days.
- Diloxanide furoate: 500 mg three times daily for 5–10 days.
Prevention and Control
- Maintain good sanitation and personal hygiene.
- Avoid faecal contamination of food.
- Ensure proper disposal of human excreta.
- Wash vegetables thoroughly before consumption.