TABLE OF CONTENTS
Leishmania donovani: Pathogenesis, Clinical Signs, Diagnosis & Treatment
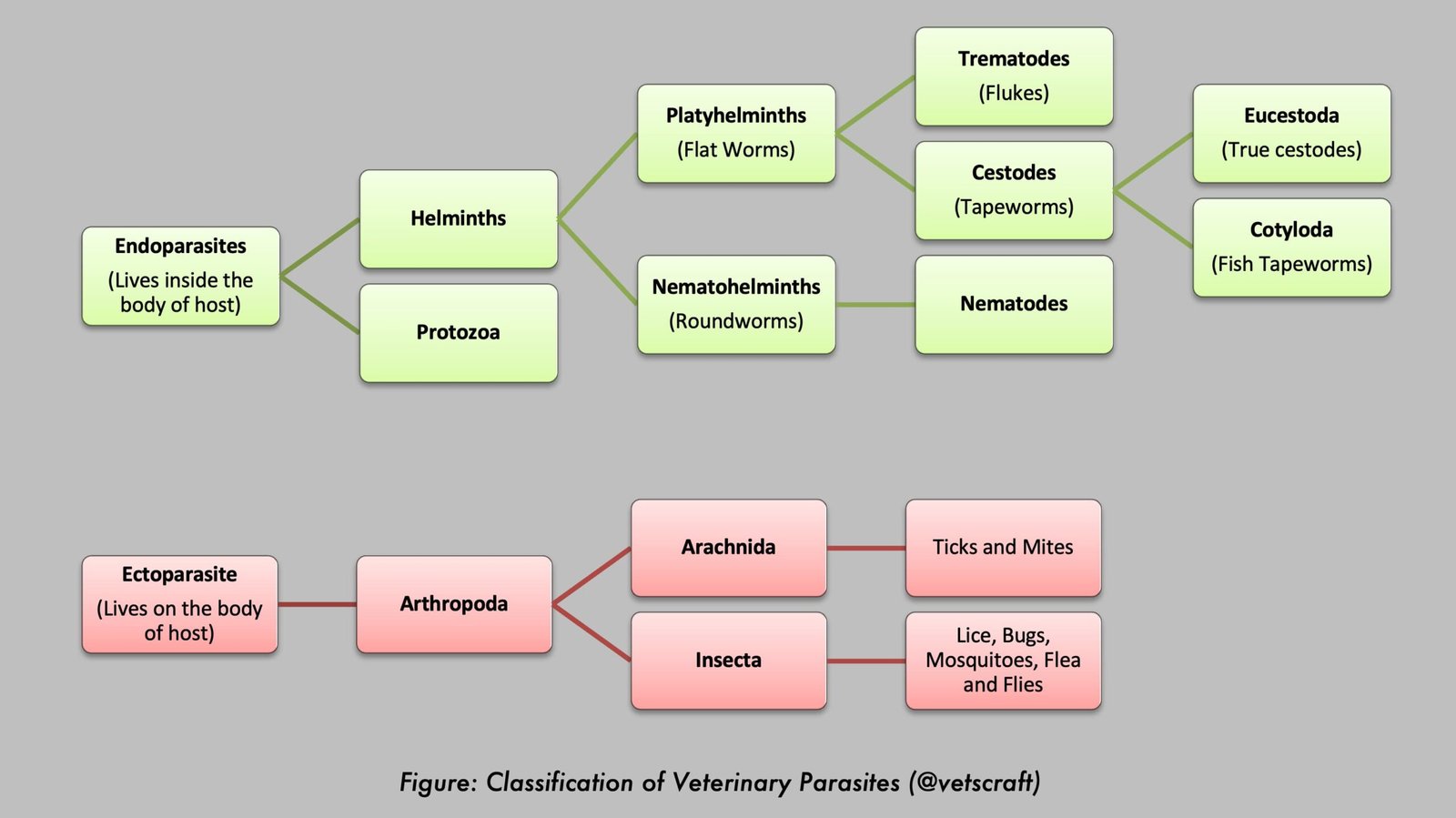
Leishmania donovani is a protozoan hemoflagellate parasite of the family Trypanosomatidae and the primary causative agent of visceral leishmaniasis (VL), also known as Kala-azar or Black fever. It is transmitted by the bite of infected female sand flies and primarily infects macrophages of the reticuloendothelial system. The parasite is of major public health importance in endemic regions of Asia, Africa, and South America.
This article provides a detailed overview of Leishmania donovani, including its taxonomical classification, pathogenesis, clinical signs in humans and dogs, postmortem lesions, post Kala-azar dermal Leishmaniasis (PKDL), diagnosis, treatment, and immunity.
Leishmania donovani causes visceral leishmaniasis (VL), Kala-azar (Black fever), and Dum Dum fever. In India, VL is not zoonotic, whereas in the Mediterranean region and China, the disease is zoonotic because dogs act as reservoir hosts; therefore, the infection is transmitted from dogs to humans.
Parasite Overview
- Vector: Phlebotomus argentipes in India
- Host: Humans and dogs are the principal hosts, but the parasite also occurs in sheep, cats, and horses.
- Distribution: India, Sudan, China, Mexico, South America, and Africa
- Disease Caused: Visceral leishmaniasis (VL), Kala-azar (Black fever), and Dum Dum fever.
Taxonomical Classification of Leishmania donovani
- Kingdom: Protista
- Phylum: Euglenozoa
- Class: Kinetoplastea
- Order: Trypanosomatida
- Family: Trypanosomatidae
- Genus: Leishmania
- Subgenus: Leishmania
- Species: Leishmania donovani
Pathogenesis
The incubation period ranges from 10 days to 1 year. Kala-azar affects people of all ages, but a higher prevalence occurs in infants and juveniles between 10 and 20 years of age. The incidence is higher in males than in females. The Indian form of visceral leishmaniasis is a highly fatal disease in humans.
Initially, the promastigotes inoculated by sand flies proliferate at the site of infection within macrophages and transform into amastigotes. Thereafter, the infected macrophages are carried through the bloodstream to internal organs such as the spleen, bone marrow, and liver, where they multiply and form clusters of organisms. During multiplication, the macrophages are destroyed.
The destruction of large numbers of macrophages may trigger compensatory production of macrophages and phagocytes. As a result, the host cellular immune mechanism becomes stimulated, and eventually bone marrow erythropoiesis is affected.
In addition, hypertrophy of the internal organs leads to suppression of blood cellular elements (RBCs and leukocytes, except monocytes). Consequently, clinical manifestations such as leukopenia, granulocytopenia, monocytosis, anemia, thrombocytopenia, lymphadenopathy, and hyperglobulinemia occur.
In advanced cases, involvement of the digestive tract may cause diarrhea, marked emaciation, abdominal distension, and a mortality rate of 70–90% in untreated cases. Death usually occurs within a few weeks to a few years after infection.
Clinical Signs in Humans
Malaise, headache, irregular intermittent fever, abdominal distension with pain, anemia, dysentery, diarrhea, edema, hyperpigmentation of the skin, bleeding from the mucous membranes of the gums, pale tongue, and enlargement of the lymph nodes.
Postmortem Lesions
- Emaciation, anemia, and enlargement of the liver and spleen
- Endothelial cells and macrophages contain masses of amastigotes.
- The lymph nodes are usually enlarged.
Clinical Signs in Dogs
L. donovani causes visceral or cutaneous leishmaniasis. The cutaneous form is more common, usually causing low mortality; however, the mortality rate may be high in acute cases. Affected dogs may exhibit anemia, cutaneous ulcers, and alopecic patches on the face, particularly around the eyes, giving the appearance that the dog is wearing spectacles.
Shallow ulcers may be observed on the lips and eyelids along with generalized eczema. Intermittent fever, cachexia, generalized lymphadenopathy, and diarrhea are important clinical signs.
PKDL (Post Kala-azar Dermal Leishmaniasis)
PKDL (Post Kala-azar Dermal Leishmaniasis) is the secondary form of Indian Kala-azar that occurs in humans (40% of Indian cases) due to incomplete therapy. Because of incomplete therapy, the amastigotes present in the viscera migrate to the skin, where they multiply and produce lesions.
This condition may occur even 7 years after recovery from the clinical disease, may persist for 1–2 years, and acts as a persistent reservoir of infection. The chronic lesions consist of multiple nodular infiltrations of the skin without ulceration.
Initially, the lesions appear as hypopigmented macules, which then develop into pea-sized nodules of varying numbers. Organisms can be demonstrated by preparing smears from the nodular material.
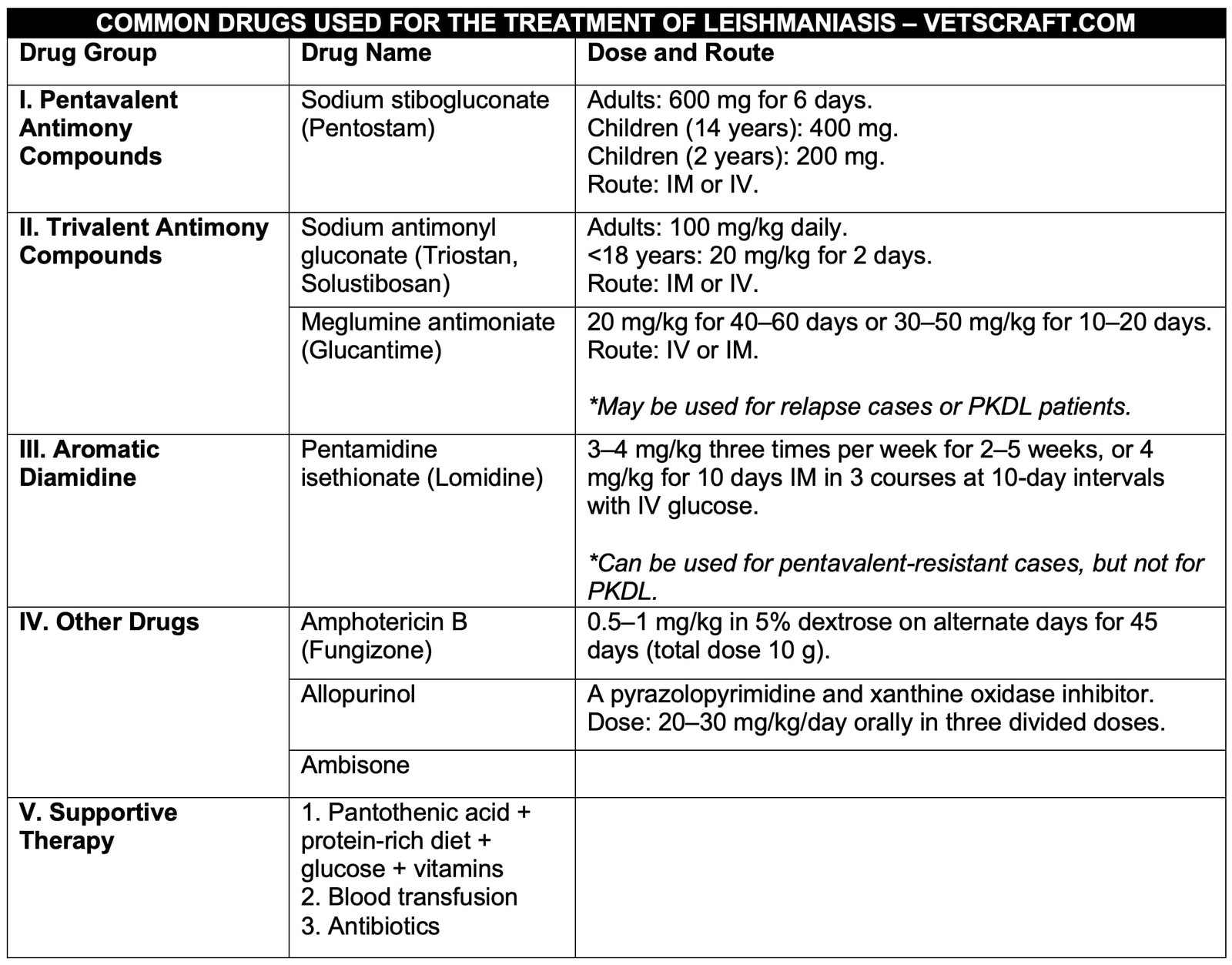
Treatment
It requires approximately twice the drug dose used for VL, and usually 4–5 courses of therapy are needed. The second course should be repeated 2 months after the first course.
Immunity
Immunity develops in incompletely treated humans, and reinfection may not occur in cured patients living in endemic areas. In dogs, only temporary clinical improvement occurs, and the parasites persist even after treatment.
Diagnosis
- Based on clinical signs and lesions
- Examination of thick and thin blood smears
- Examination of buffy coat smears
- Examination of deep skin scrapings collected from the edges of the lesions, followed by staining
- Biopsy specimens may be obtained from the spleen, liver, lymph nodes, and bone marrow. Sternal or iliac crest bone marrow puncture is commonly practiced in humans.
- Culture of the collected material in NNN (Novy–MacNeal–Nicolle) medium
- Hematology: leukopenia, monocytosis, and anemia
- Animal inoculation: Golden hamsters are used. Suspected material is inoculated via the intracardiac route. In positive cases, the internal organs become heavily parasitized within 2 weeks.
Non-specific tests for diagnosis:
- Napier aldehyde test
- Chopra’s antimony test
- CFT, PHA, and IHA
Treatment
Generally, the response to treatment in dogs is poor. However, Solustibosan may be used instead of Pentostam.