TABLE OF CONTENTS
Giardia lamblia: Morphology, Life Cycle, Pathogenesis, Diagnosis, Treatment & Control
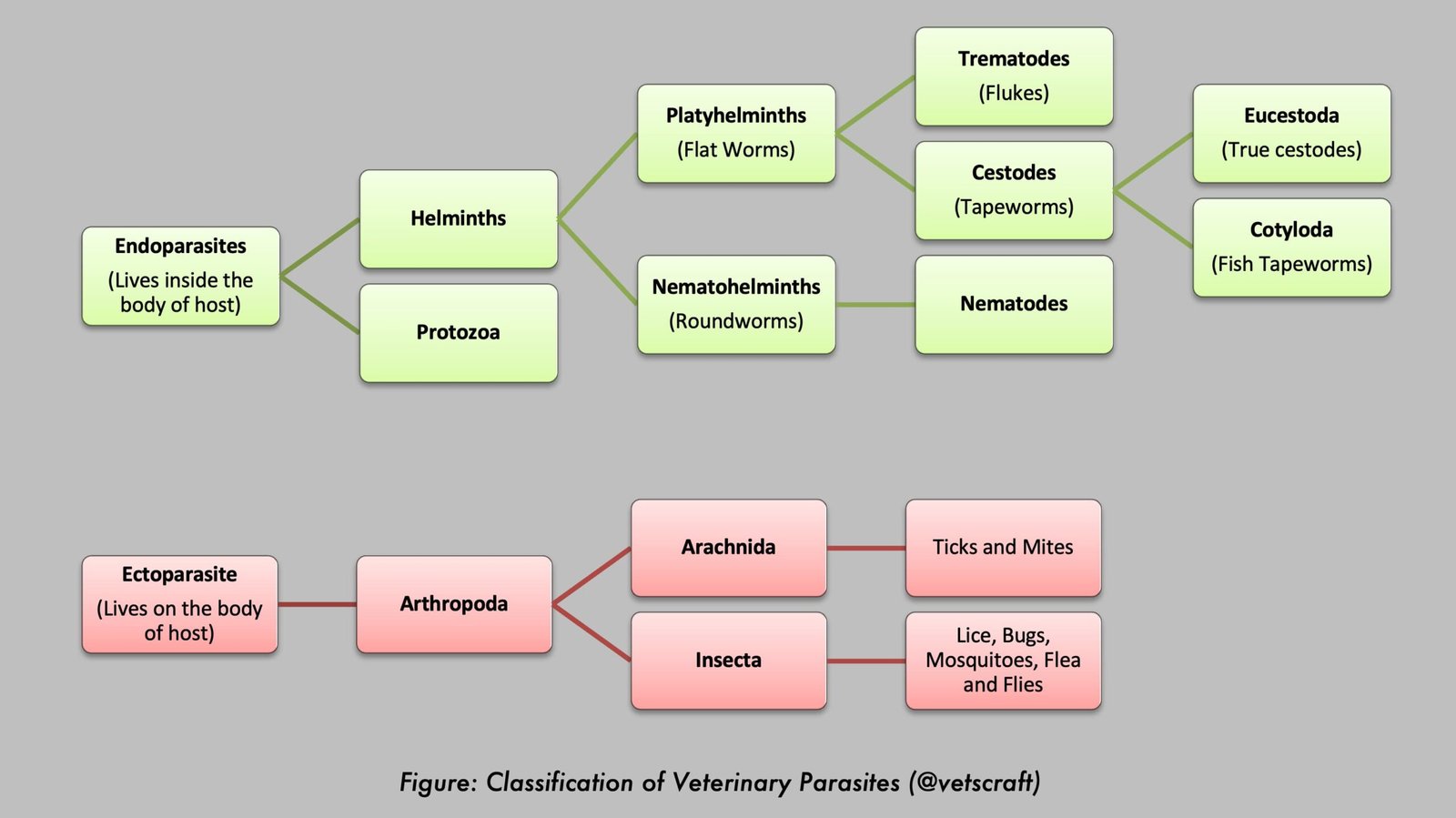
Giardia lamblia (also known as Giardia intestinalis or Giardia duodenalis) is a flagellated protozoan parasite that infects the small intestine of humans and a wide range of mammals. It is one of the most common intestinal parasites worldwide and is a major cause of waterborne and foodborne diarrheal disease, particularly in areas with inadequate sanitation and contaminated drinking water.
Infection with Giardia lamblia, known as giardiasis, ranges from asymptomatic carriage to acute or chronic gastrointestinal illness characterized by diarrhea, abdominal discomfort, malabsorption, and weight loss.
Parasite Overview
- Host: Humans
- Predilection Site: Duodenum and other parts of the small intestine; occasionally found in the colon.
- Disease Caused: Traveler’s diarrhea (Giardiasis)
- Distribution: Cosmopolitan; commonly occurs in warm climates.
Taxonomical Classification
- Kingdom: Protista
- Phylum: Metamonada
- Class: Fornicata
- Order: Diplomonadida
- Family: Hexamitidae
- Genus: Giardia
- Species: Giardia lamblia
- Common Name: Giardia, intestinal giardia
Members of the family Hexamitidae are easily recognized by the presence of two nuclei lying side by side. Of the five genera in this family, the genus Giardia is the most important, affecting almost all animal species, including humans. Different names have been given based on the host from which it was identified.
Giardia lamblia or G. intestinalis (humans) was first discovered in 1681 by Antoni van Leeuwenhoek in his own stool. Other species in this genus include G. bovis (cattle), G. canis (dog), G. cati (cat), and G. muris (rat).
Morphology
The trophozoite is pyriform to elliptical in shape and bilaterally symmetrical. The anterior end is broadly rounded, and the posterior end is pointed.
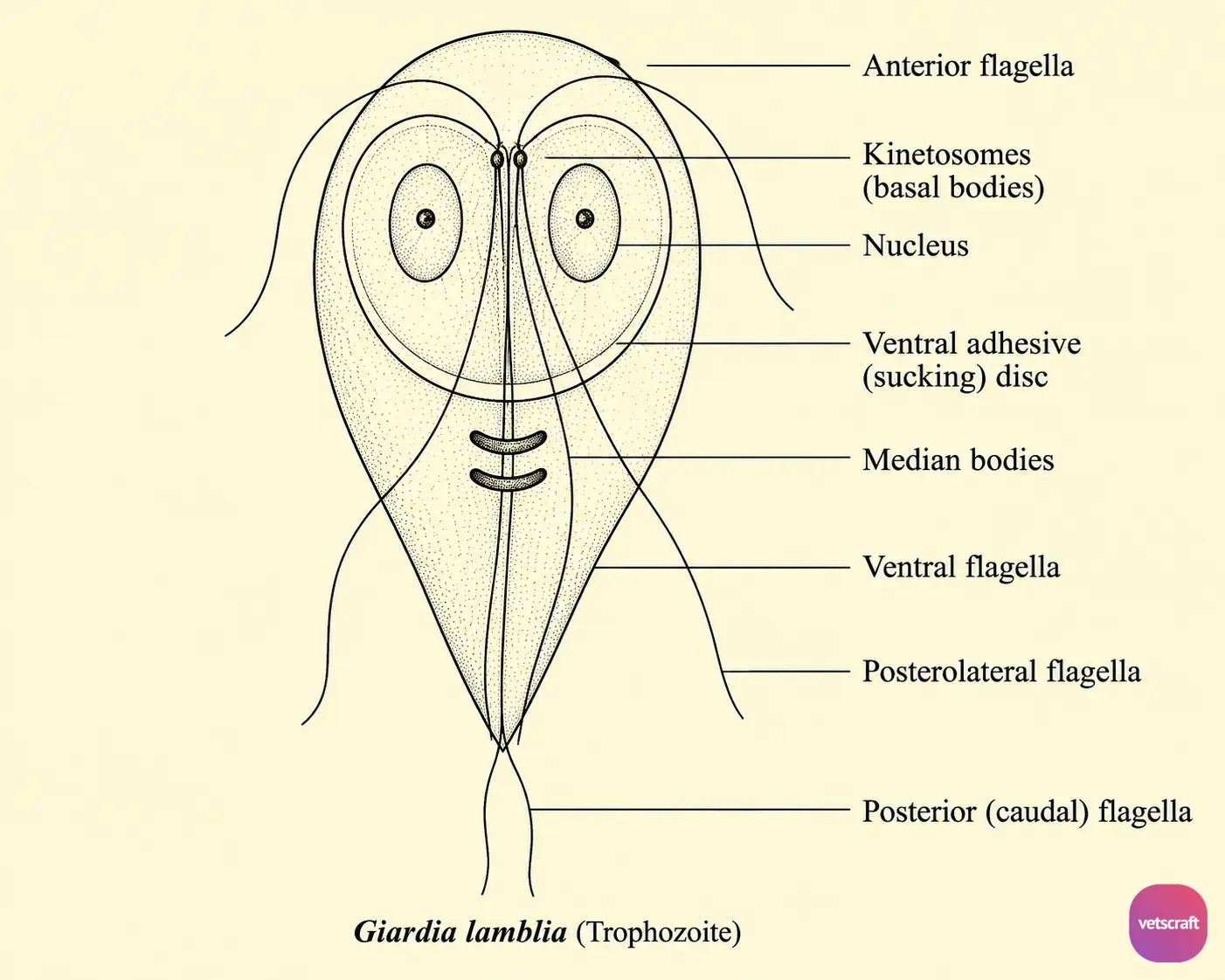
The ventral surface is concave and bears a large sucking disc called the adhesive disc, while the dorsal surface is convex. A pair of ventral flagella and three pairs of anterior flagella arise from the kinetosomes located between the anterior margins of the two nuclei.
A pair of large, curved, transversely oriented, darkly staining bodies located behind the adhesive disc are called the median bodies. The ventral flagella and ventral groove help the organism firmly adhere to the host cells.
There is no true axostyle, but a tube-like structure called the ventral groove, composed of microtubules, is present.
Cyst
The cyst has two or four nuclei, giving the appearance of a pair of spectacles, along with a number of fibrillar remnants of the trophozoite organelles such as the median bodies and axostyle.
Transmission and Life Cycle
Giardiasis is mainly transmitted through the ingestion of cysts in contaminated water or food. The ingested cysts safely pass through the stomach and undergo excystation in the duodenum. Following this, trophozoites are released and multiply by longitudinal binary fission.
During multiplication:
Nuclei divide first → Locomotory apparatus divides → Sucking disc divides → Cytoplasm divides → Large numbers of trophozoites are produced.
Trophozoites are found only in watery stools and in the small intestine. They become encysted when the intestinal contents enter the colon because of increased water absorption in the large intestine. Young cysts contain two nuclei, which increase to four as the cysts mature.
The cysts are ovoid, with duplicated sucking discs and locomotory apparatus, and are passed in the feces. Mature cysts are the infective stage for susceptible hosts.
Epidemiology
Giardiasis is highly contagious. If one person in a household becomes infected, other members may also become infected within a few days. Children are more susceptible.
Pathogenesis and Clinical Signs
G. lamblia lives in the duodenum, jejunum, and upper ileum with the help of its adhesive disc. The trophozoites usually lie flat on the surface of the epithelial cells.
In many cases, the infection may go unnoticed, whereas in some cases it causes clinical signs such as excessive mucus production, diarrhea, dehydration, abdominal pain, flatulence, and weight loss.
In severe infections, the free surface of every epithelial cell may become covered with trophozoites. This can interfere with fat absorption, resulting in fatty stools (steatorrhea). Because of impaired fat absorption, deficiencies of fat-soluble vitamins may occur.
Diagnosis
- Demonstration of Cysts in Fecal Material: Cysts are usually passed in well-formed feces. They can be concentrated by flotation using 33% zinc sulfate solution. While examining the flotation material, a small quantity of iodine solution may be added to facilitate recognition of the cysts.
- Demonstration of Trophozoites: Trophozoites may also be passed in the feces during acute diarrheal cases. Therefore, diarrheic feces can be examined by direct microscopic examination for the demonstration of trophozoites.
Treatment
- Metronidazole: 250 mg orally three times daily for 5–7 days
- Quinacrine: 100 mg orally three times daily for 5–7 days
- Tinidazole: 2 g orally as a single dose
- Mepacrine: 100 mg orally three times daily for 5–7 days
Control
Hot water should be used for drinking purposes.