TABLE OF CONTENTS
Dicrocoelium dendriticum (Lancet Liver Fluke): Morphology, Life Cycle, Pathogenesis, Diagnosis & Treatment
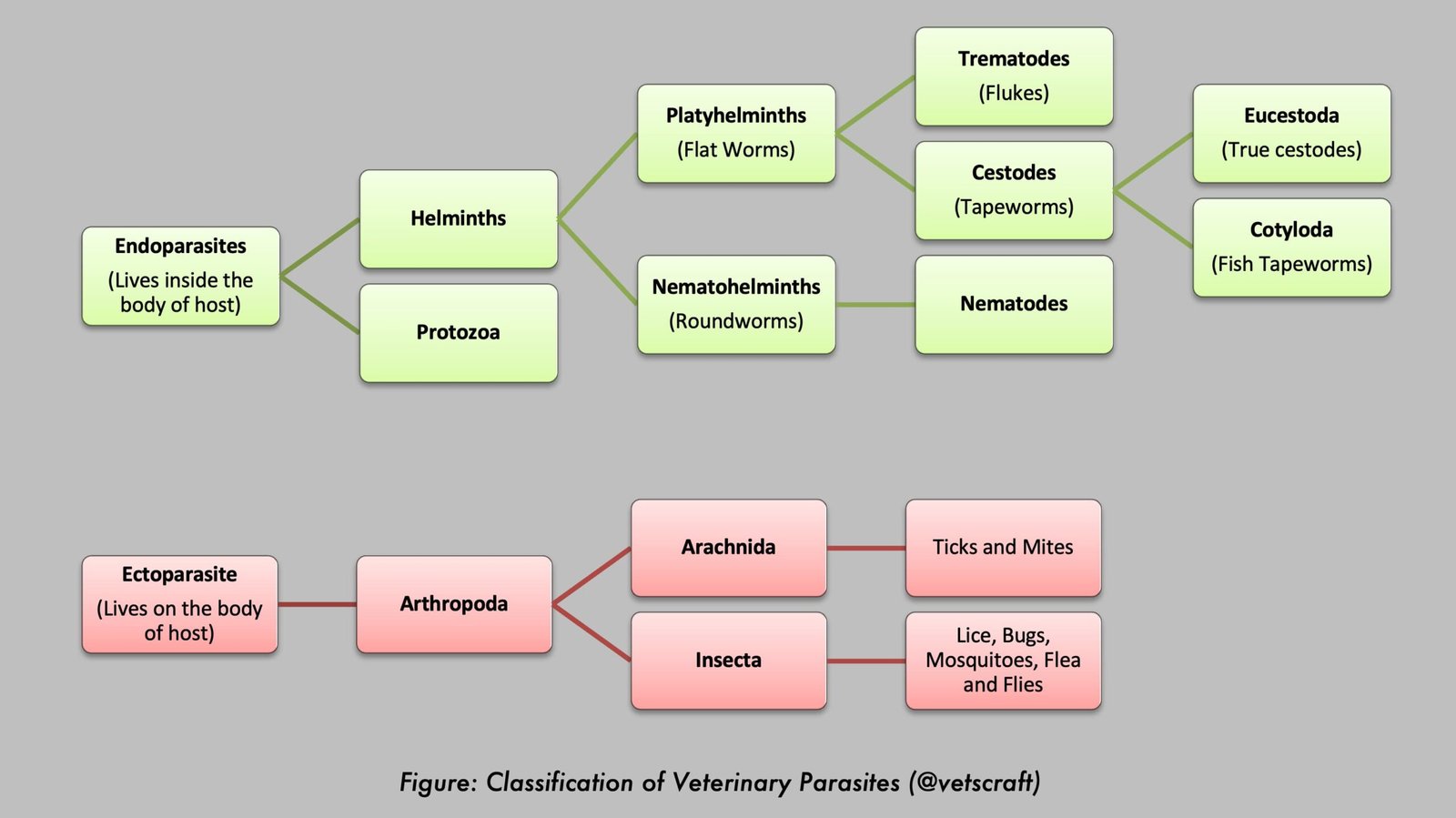
Dicrocoelium dendriticum, commonly known as the lancet liver fluke, is a trematode parasite that infects the bile ducts of ruminants and other mammals worldwide. Unlike Fasciola species, this parasite does not migrate through the liver parenchyma, resulting in a distinct pathogenesis and life cycle involving land snails and ants as intermediate hosts.
Taxonomical Classification
- Family: Dicrocoeliidae
- Genus: Dicrocoelium
- Species: D. dendriticum (Synonym: D. lanceolatum)
- Common Name: Lancet fluke
- Hosts: Sheep, goats, cattle, deer, pigs, dogs, donkeys, rabbits, and rats. It rarely infects humans.
- Location: Bile ducts and gallbladder.
- Intermediate Hosts (I/H):
- 1st I/H: Land snails (e.g., Macrochlamys cassida, Zebrina detrita, Cionella lubrica)
- 2nd I/H: Brown ant (Formica fusca)
- Distribution: Worldwide
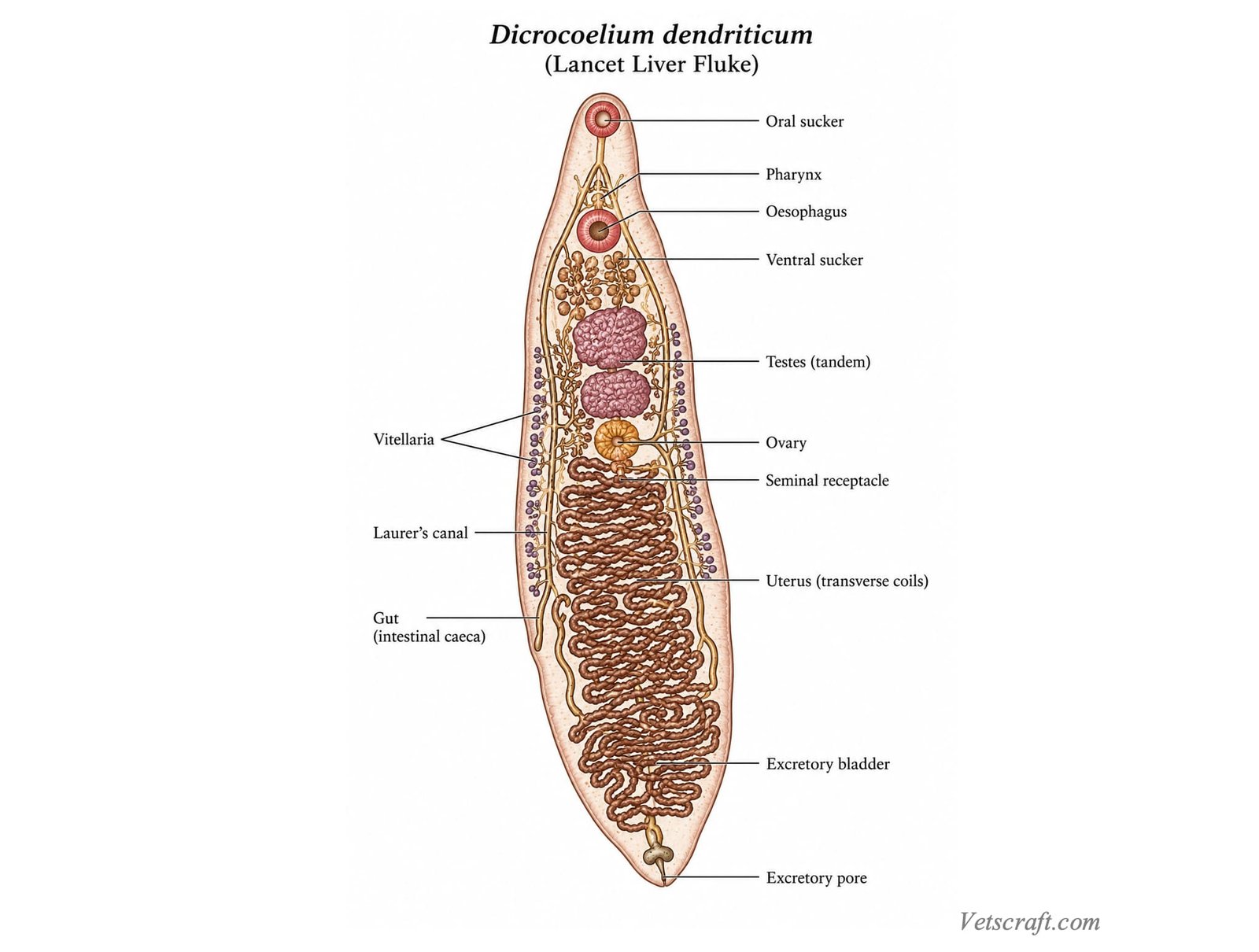
Morphology
- Dicrocoelium dendriticum is 6–10 mm long and 1.5–2.5 mm wide.
- Lancet-shaped (lanceolate), elongated, narrow anteriorly, and widest behind the middle.
- The cuticle is smooth.
- The oral sucker (OS) is smaller than the ventral sucker (VS) and both are located in the anterior one-third of the body.
- A pharynx and esophagus are present. The intestinal ceca are simple, bifurcated like a tuning fork, and do not reach the posterior end.
- The excretory bladder is simple and tubular.
- The testes are slightly lobed and lie almost in tandem immediately posterior to the ventral sucker.
- The ovary lies posterior to the testes.
- The vitelline glands occupy the middle third of the lateral fields and appear whitish in color.
- The space behind the gonads is occupied by transverse coils of the uterus, which appear dark brown in color.
- Eggs are dark brown, operculated, and embryonated when laid (containing a miracidium).
Life Cycle
- The eggs do not hatch until they are ingested by the first intermediate host (snail).
- The eggs hatch in the snail’s gut, and the liberated miracidia migrate to the mesenteric gland, where they develop into polymorphous sporocysts (mother sporocysts), which lack a distinct cuticle.
- These produce second-generation sporocysts (daughter sporocysts) with a cuticle and birth pore, which in turn produce cercariae (the stylet-bearing cercaria, Cercaria vitrina, is known as a xiphidiocercous cercaria).
- The redial stage is absent. Cercarial development takes approximately 3 months.
- Cercariae emerge from the sporocysts only during damp weather following a dry period.
- Within the pulmonary chamber of the snail, cercariae aggregate into masses called “slime balls.” Each slime ball contains 200–400 cercariae embedded in a thick gelatinous substance. They are expelled by the snail following a drop in temperature and adhere to vegetation.
- The slime balls are consumed by brown ants (Formica fusca), and metacercariae develop within the body cavity of the ant in approximately 26–62 days.
- Some metacercariae migrate to the ant’s brain, causing tetanic spasms of the mouthparts and lethargy. Affected ants attach themselves to herbage available to grazing animals during the early morning.
- The definitive host becomes infected by ingesting infected ants along with herbage.
- Following ingestion of infected ants, excystation occurs in the small intestine. The liberated juvenile flukes enter the intestinal opening of the common bile duct and migrate into the smaller bile ducts of the liver. There is no migration through the liver parenchyma. The prepatent period is 47–54 days.
Pathogenesis
The small flukes penetrate the branches of the bile ducts, causing marked dilation and attaching to the duct walls by means of their suckers.
Several thousand flukes may be present within the bile ducts, yet the liver remains relatively normal because there is no migration through the hepatic parenchyma.
In severe infections, postmortem lesions include:
- Extensive fibrosis (cirrhosis) and edema.
- Scarring of the liver surface.
- Marked dilation and distension of the bile ducts with large numbers of flukes.
- Marked proliferation of the bile duct epithelium.
- Early fibrosis in the portal areas that later extends in an interlobular and perilobular pattern, producing lesions similar to cirrhosis.
- The disease condition is known as “Dicrocoeliosis.”
Clinical Signs
Clinical signs are generally absent. However, in severe infections, anemia, hypoproteinemia, edema, poor growth, emaciation, and weight loss may occur. Significant economic losses may result from liver condemnation when large numbers of flukes are present in the bile ducts.
Diagnosis
Diagnosis is based on fecal examination and necropsy findings.
Treatment
- Hetolin (Methyl Piperazine Derivative): 19–22 mg/kg body weight
- Diamphenethide: 300 mg/kg body weight
- Albendazole: 15 mg/kg or 7.5 mg/kg body weight in two doses administered 2–3 weeks apart
- Cambendazole: 25 mg/kg body weight
- Fenbendazole: 150 mg/kg body weight
- Thiabendazole: 200–300 mg/kg body weight
- Praziquantel: 50 mg/kg body weight
- Thiophanate: 50 mg/kg body weight
- More recently, Netobimin (20 mg/kg) has been found to be highly effective.
High doses are frequently required. Generally, doses approximately three times higher than those used for nematode infections are needed, making treatment relatively uneconomical.
Control
- Treatment of infected animals.
- Control of snail and ant populations.
Control is difficult because of the widespread distribution of intermediate hosts and the involvement of numerous wild animals that serve as reservoir hosts.