TABLE OF CONTENTS
Bio-transformation of drugs
The chemical alteration of drugs in the body
- To render nonpolar lipid soluble compounds into polar water soluble compounds to enhance their excretion from the body
- Intended to protect body from the foreign substances by making them less toxic and easily excreted
- Primary site – liver
- Other important sites are kidney, intestine, lungs and plasma
Sequelae of biotransformation reactions
- Inactivation – most drugs arerendered pharmacologically inactive. Example: Many drugs – morphine, chloramphenicol, procaine etc.
- Formation of active metabolite – the metabolite formed possesses biological activity
- Ciprofloxacin from enrofloxacin
- Oxyphenbutazone from Phenylbutazone
- Salicylic acid from aspirin
- Inactive drug to active drug (Prodrug) An inactive drug gets converted into an active metabolite once it undergoes biotransformation inside the body. Example: Hetacillin to ampicillin and Prontosil to sulfanilamide.
- Less active or inactive drug is converted into a more toxic drug (Lethal synthesis). Example: Parathion to paraoxon and Fluoroacetic acid to fluorocitrate.
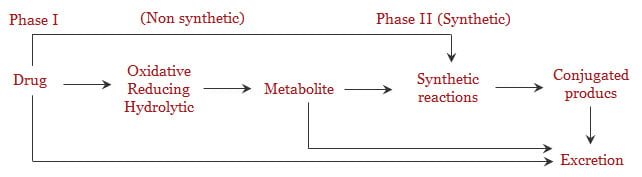
General Pattern of biotransformation is biphasic. these phase 1 and phase 2 described below-
1. Phase-I Biotransformation – oxidation reactions and others
Although every tissue has some ability to metabolize drugs, the liver is the principal organ of drug metabolism. Other tissues that display considerable activity include the gastrointestinal tract, the lungs, the skin and the kidneys.
Drug biotransformation in vivo can occur by spontaneous, noncatalysed chemical reactions (Hofmann degradation), which however is very rare.
The vast majority of xenobiotics undergo biotransformation the reactions of which are catalysed by specific cellular enzymes. At the subcellular levels, these enzymes may be located in the endoplasmic reticulum, mitochondria, cytosol, lysosomes or even the nuclear envelope or plasma membrane.
Many drug metabolising enzymes are located in the lipophilic membranes of the endoplasmic reticulum of the liver and other tissues. When these lamellar membranes are isolated, they re-form into vesicles called microsomes. The rough microsomes tend to be dedicated to protein synthesis and the smooth microsomes are relatively rich in enzymes responsible for oxidative drug metabolism. They contain the important class of enzymes known as the Mixed Function Oxidases or monooxygenases or CYP 450 enzymes (Cytochrome P450 enzyme system)
Microsomal enzymes / mixed function oxidases
- catalyse oxidative and glucuronide conjugation reactions
- Requires molecular O2, CYP 450 ( a heme protein), NADPH (reduced nicotinamide adenine dinucleotide phosphate )
- NADPH + CYP 450 (A)+H+ AH2 + NADP+
- AH2 + O2 ‘active oxygen complex’
- Drug + ‘active oxygen complex’ oxidized drug + A + H2O
Phase I reactions
| Reaction | Example |
| Oxidative reactions | |
| N- and O- dealkylation | phenacetin, morphine |
| Aliphatic and aromatic hydroxylation | Phenobarbital, phenytoin |
| N-Oxidation | Guanethidine, acetaminophen |
| Sulphoxide formation | Chlorpromazine |
| Deamination of amine | Amphetamine |
| Desulfuration | Thiobarbital, parathion |
| Hydrolysis of esters and amides | Procaine |
| Reduction | |
| a. Azo reduction | Prontosil |
| b. Nitro reduction hloramphenicol | Chloramphenicol |
2. Phase-II reactions – Synthetic reactions
Conjugation of a functional group to the drug or its metabolite to make it water soluble. The presence of –OH, -COOH, -NH2, -SH groups favour formation of conjugates (these groups are added to (or) exposed in Phase I)
Glucuronidation
- The most important reaction – most drugs incl. endogenous steroids and bile pigments undergo this reaction.
- Glucuronide conjugation takes place in microsomes.
- The source of glucuronide is UDPGA through glucuronyl transferase.
- The product is highly soluble and is excreted by urine (if MW<300 – 500) or via bile ( if >500)
- Beta -glucuronidase in intestine may liberate the active drug which is again reabsorbed and undergoes enterohepatic recirculation which leads to longer duration of action of the drug
Sulfate conjugation (non-microsomal)
- Forms ethereal sulfates – eg. Phenols, acetaminophen, morphine and endogenous heparin, chondroitin and some steroids
Acetylation (non microsomal)
- Acetylates are formed eg. Sulphonamides — acetyl CoA is the donor
- Acetylates are poorly soluble in water and lipid and are likely to cause crystalluria
Methylation (non-microsomal)
- Adds methyl radicals – The aminoacids methionine and cysteine are the donors
- eg. Histamine, adrenaline, sex steroids
Glycine conjugation (non-microsomal)
- Not a major pathway, eg. Salicylates
Glutathione conjugation
- Not a major pathway – forms mercapturic acids – important for removal of toxic radicals (superoxides, epoxides and toxic intermediates)
Ribonucleoside / Ribonucleotide synthesis
Ribonucleotide synthesis reactions are important for the activation of purine and pyrimidine anti-metbolites used in cancer therapy
Drug conjugates were once believed to represent terminal inactivation events and as such have been viewed as “true detoxification” reactions.
However, this concept must be modified, since it is now known that certain conjugation reactions may lead to the formation of reactive species responsible for the hepatotoxicity of the drug.
Enzyme induction and inhibition
Enzyme inhibition
Some drugs on repeated administration have the ability to “inhibit” cytochrome P-450 enzyme activity. These drugs cause a reduction in the metabolism of other drugs that are administered subsequently.
Some drugs that act as inhibitors are chloramphenicol, cimetidine, dicumarol, oral contraceptives, ethanol and isoniazid. This is an immediate process due to direct inhibition of the enzyme or competition among drugs for the enzyme site. As a result the concentration of drug increases leading to increased drug effect
Enzyme induction or stimulation
Some drugs on repeated administration have the ability to “induce” cytochrome P-450 by enhancing its rate of synthesis or by reducing its rate of degradation.
Induction results in an acceleration of metabolism and usually in a decrease in the pharmacologic action of the inducer and also of coadministered drugs.
Increase in enzyme concentration due to induction of protein synthesis ( hence called INDUCERS) and takes long time to set in and once the inducing drug is stopped, takes long time to return to original values.
Some drugs that act as inducers are griseofulvin, phenobarbital, phenylbutazone, phenytoin and rifampin.
Significance of enzyme induction / inhibition
- Inhibitors prolong the activity of co-administered drugs
- It also increases the toxic effects of unchanged drugs, if any
- Drug metabolism varies in smokers and alcoholics ( in human patients)
- In case of combined administration, alteration of dose may be required
Factors affecting biotransformation of drugs
- Age: Biotransformation is poor in neonates since enzyme systems are not well developed. Biotransformation is poor in old animals, too
- Disease: Diseases of the liver- hepatitis, cirrhosis etc.. and also diseases causing low blood flow to liver such as CHF, shock etc. will alter biotransformation
- Species differences:
- Cats are deficient in glucuronidation (low level of glucuronyl transferase)
- Dogs lack acetylation
- Pigs have low capacity for sulfation
- Genetic differences do exist in human racesin metabolizing many drugs ( eg.. metoprolol in man)
- Losartan – an antihypertensive – effective in man but less so in dogs since the active metabolite is not formed in dogs
- Rabbits possess atropinase – therefore do not suffer from toxicity due to atropine (in deadly night shade poisoning)
- Co-administration of other drugs – inducer or inhibitor
- Habits like alcoholism and smoking or industrial pollutants, pesticides may alter metabolism of some drugs
First pass metabolism
- Refers to the process of metabolism of a drug before it reaches systemic circulation.
- Normally happens in drugs administered by oral route. Besides oral route, it can occur in topical (skin) and lungs, too (however at low levels)
- Effects of first pass metabolism:
- Increased oral dose of the drug
- Unpredictable absorption of oral dose variation among individuals in drug action
- Oral bioavailability increased, if there is liver disease
Enterohepatic recirculation
Some drugs after biotransformation by glucuronide conjugation, undergo biliary excretion. In the large intestine they are detached from the conjugate, leading to release of free drug which is absorbed again and enters liver. Thus the drug recirculates leading to longer duration of action. Eg: Phenalpthaelin used as purgative.