TABLE OF CONTENTS
Ovariohysterectomy (OHE) in Dogs: Indications, Approaches, Procedure and Complications
Ovariohysterectomy (OHE) is a surgical procedure performed on female dogs that involves the removal of both the ovaries and the uterus.
Ovariohysterectomy (OHE) commonly known as spaying, this procedure is done to prevent unwanted pregnancies, stop the dog’s heat cycles, and reduce the risk of uterine infections, ovarian tumors, and breast cancer in the long term.
Indications
- Prevention of unwanted pregnancy
- Elimination of heat cycles
- Reduction of reproductive cancer risk (ovarian, uterine, and mammary tumors)
- Prevention of pyometra
- Behavioral benefits (reduction in aggression and heat-related behaviors)
- Improved longevity and health
- Management of medical conditions (uterine infections, endometrial hyperplasia, cystic ovaries)
- Prevention of male dog attraction during heat
Approaches of Surgery
Common approaches of surgery for spaying (especially in female dogs):
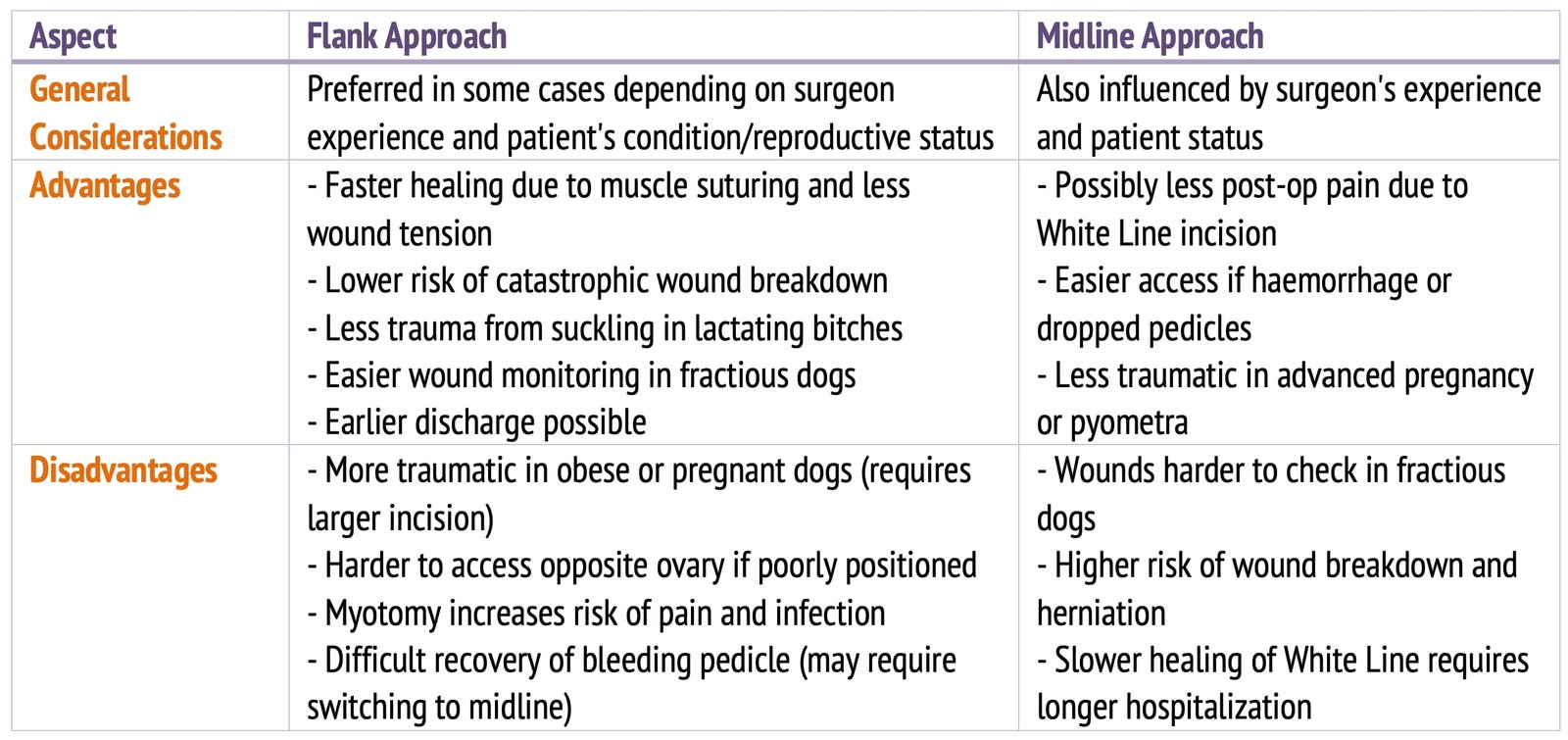
- Flank Approach
- Midline Approach
Ovariohysterectomy Procedure (Mid Ventral Approach)
The bitch is placed in dorsal recumbency, and the skin is incised along the linea alba, the sheath of the rectus abdominis, starting at the umbilicus and extending a few centimetres cranial to the pubis. Using scissors, the subcutaneous connective tissue, which may contain a substantial amount of fat, is bluntly dissected to expose the linea alba (Fig. 1).
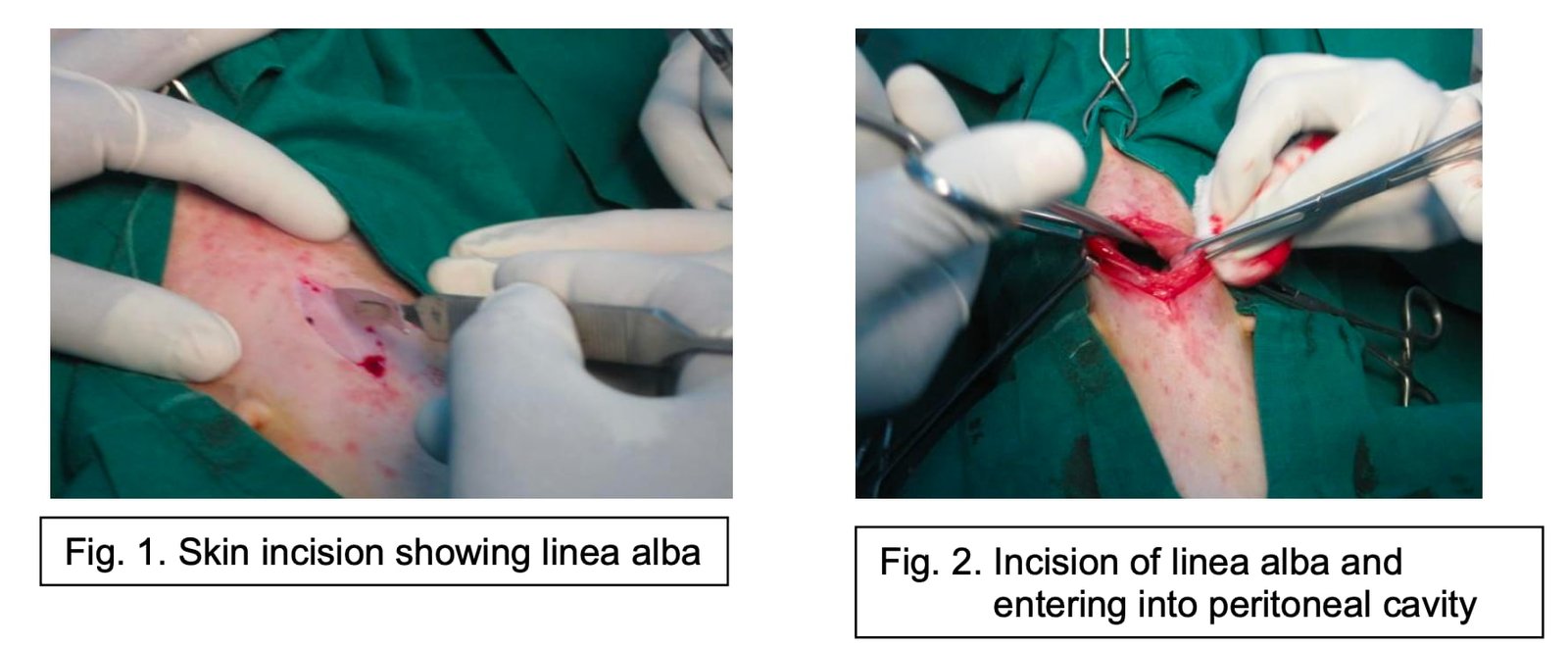
Haemostasis is performed before opening the abdominal cavity. If simple swabbing proves insufficient, any bleeders should be ligated or twisted to obtain a very clean surgical field. Using rat-tooth forceps, the linea alba is grasped in the middle and tented up before being incised with a pair of scissors.
The peritoneum is then punctured using a cannula that is slid towards the umbilicus to enable incision of the linea alba without damaging the abdominal contents, with the cutting edge of the blade turned uppermost (Fig. 2). The same procedure is then performed in the opposite direction towards the pubis.
If the uterine horns are enlarged, they will be visible at the bottom of the surgical field after incising the peritoneum. Normal-sized horns, however—such as those seen following recovery from post-oestral metritis or during routine spaying—are typically not visible. To facilitate identification of the uterine horns, the operating table is tilted so that the animal’s head is positioned lower than its hindlimbs. This position, known as the Trendelenburg position, shifts the abdominal organs cranially toward the diaphragm.
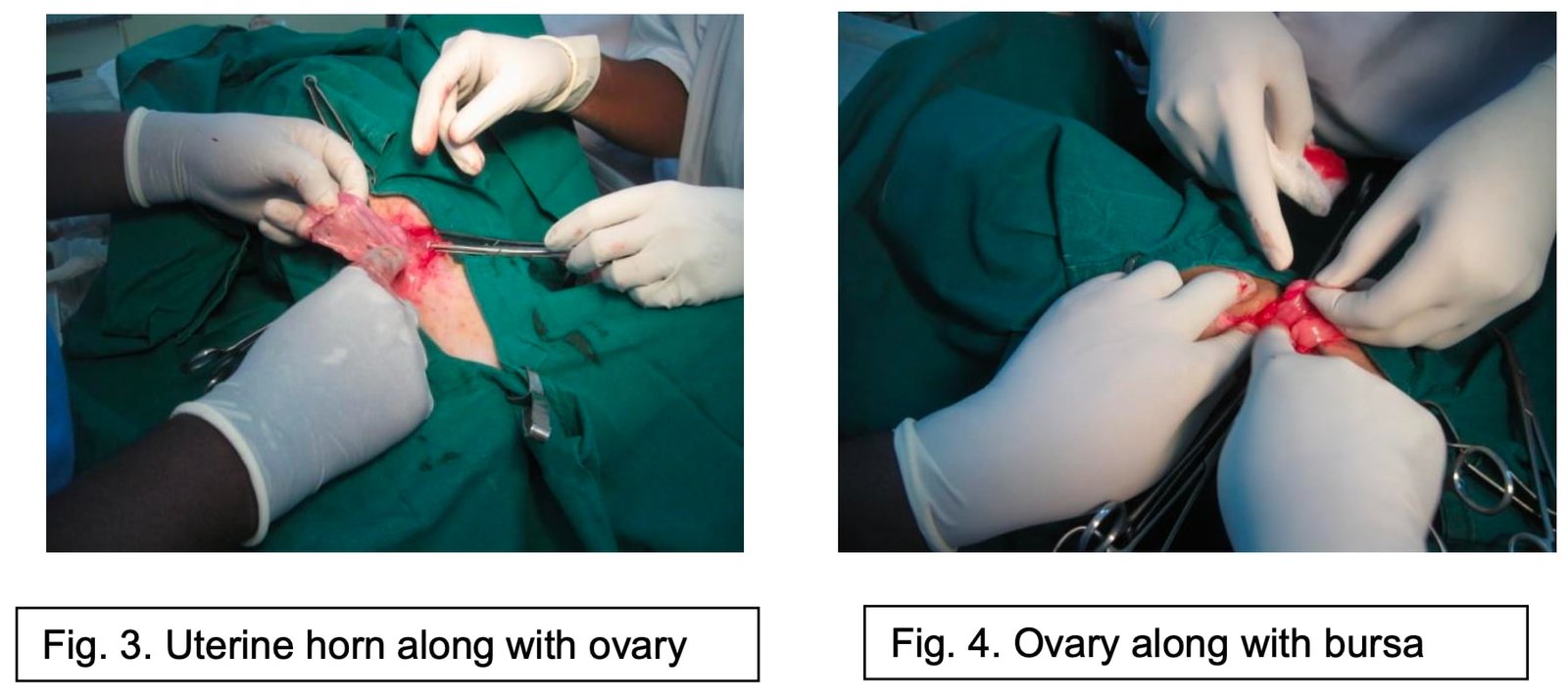
To locate the genital tract more easily, the urinary bladder is gently retracted laterally. Cranial to the bladder, the uterine body and bifurcation of the horns can be readily identified. One horn is then traced cranially to the ovary, which lies hidden within the fat-filled ovarian bursa (Fig. 3). Although the ovary is not initially visible, it can be palpated through the bursa. It is a 1–2 cm long structure that becomes visible upon incision of the bursa (Fig. 4).
Sectioning the Ovarian Pedicle
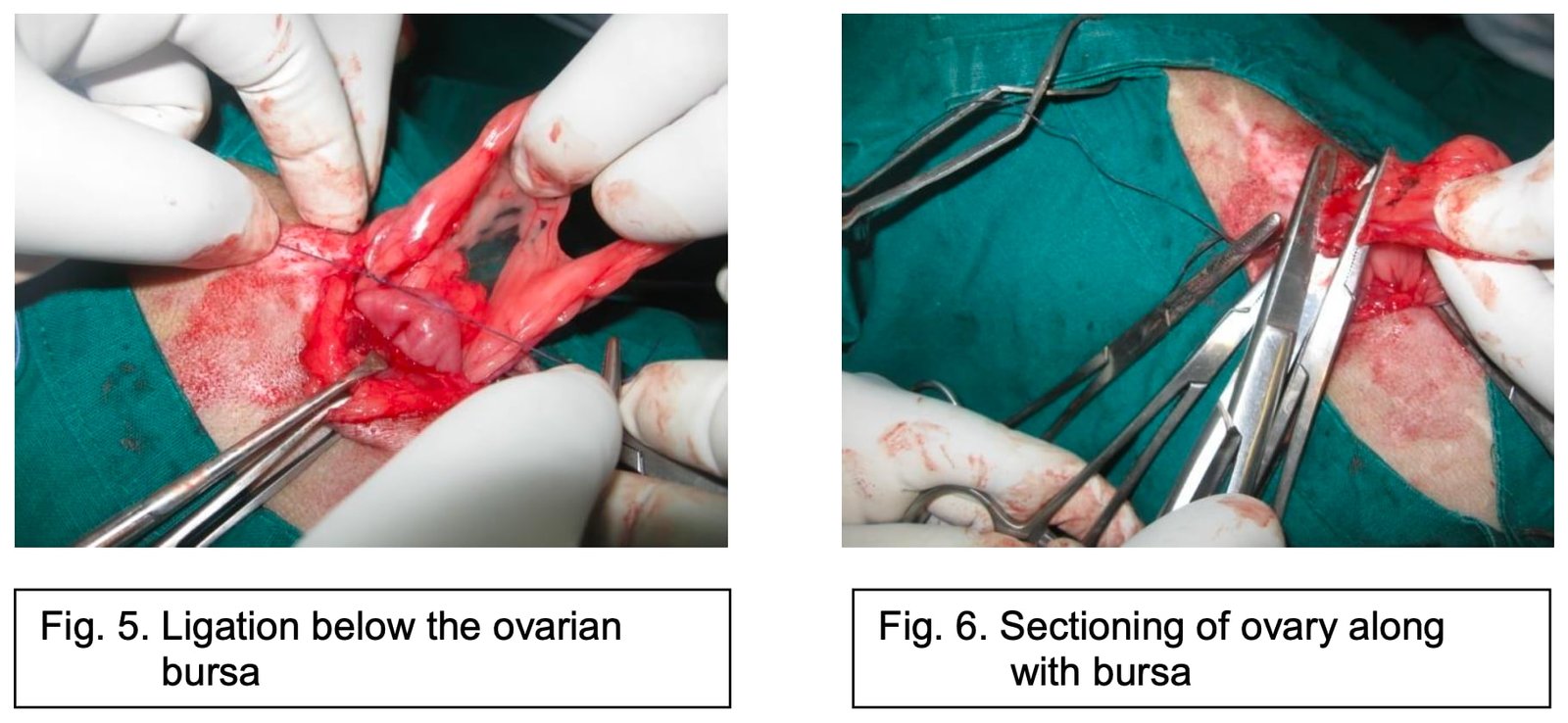
The ovary is grasped, and artery forceps are applied. These are handed to an assistant, who holds the ovarian pedicle taut outside the abdomen to facilitate placement of a ligature as close as possible to the base of the pedicle, ensuring haemostasis of the ovarian artery. The broad ligament is then punctured with a clamp to grasp the suture material, and a ligature is placed around the ovarian pedicle, as close as possible to the lumbar wall (Fig. 5). Once the ligature is secured, the suture ends are left long to allow easy identification of the pedicle in case of postoperative haemorrhage.
A second clamp is placed between the ligature and the ovary, and the pedicle is transected between the two clamps (Fig. 6). The ovarian pedicle remains clamped throughout this procedure. Haemostasis is then carefully assessed, and the long suture ends are trimmed. In some cases—such as when the vascular bundle is hypertrophied—it may be advisable to place two ligatures: one around the artery and another around the ovarian vein. The ligature itself should never be clamped, as this may cause it to slip off the pedicle during reintroduction into the abdomen.
Sectioning the Broad Ligament
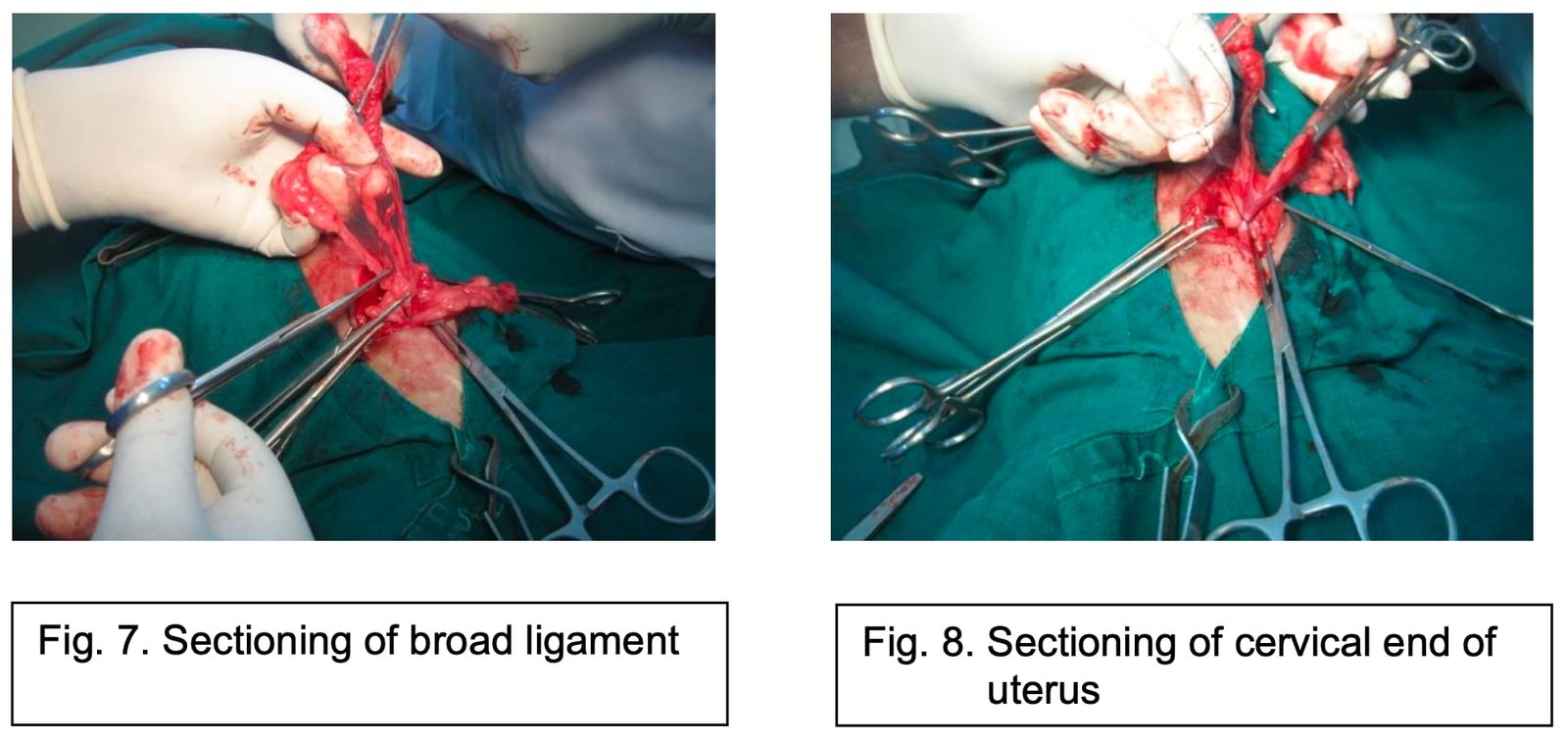
If the broad ligament contains large blood vessels, these should be ligated before being transected (Fig. 7). However, if the vessels are not visible and are buried within fat, the ligament can be manually torn in the middle, above the uterine artery, by applying traction between two swabs using the fingers. This tear is made from cranial to caudal, down to the level of the cervix and as close as possible to the lumbar wall. A point of resistance is typically encountered within the round ligament; this corresponds to the vaginal process (analogous to the scrotum in the male), which explains the risk of inguinal herniation of the uterus in bitches if this structure relaxes postoperatively.
An alternative technique for transecting the broad ligament involves placing a row of overlapping mattress sutures along its length before sectioning it with a scalpel or scissors. Once the first ovarian pedicle has been transected, the second uterine horn is located, and its corresponding ovarian bursa is grasped with artery forceps. The ovarian pedicle and broad ligament on this side are then managed as previously described. Finally, both uterine horns are returned to the pelvic cavity.
Suturing the Anterior Portion of the Laparotomy Incision
The prolapse of intestinal loops through the incision can cause significant heat and fluid loss, which can have very serious consequences, especially if the bitch is already suffering from deterioration in general status due to severe pyometria, for example. It is therefore advisable to suture the anterior portion of the laparotomy wound before continuing the surgery. However, if the haemostasis of the ovarian pedicles or broad ligaments is a source of concern, the placement of a few forceps should suffice to provide temporary closure of the anterior portion of the laparotomy wound.
Sectioning the Cervix
Once both uterine horns have been flipped back onto the pelvis, the uterine cervix is sectioned (Fig. 8), following ligation of the uterine arteries and veins. The veins can be visualised passing on either side of the cervix. The arteries run under the veins in the musculosa of the cervix, which is why the haemostatic sutures should transfix the lateral walls of the cervix. However, if the uterine artery is perforated during ligation, a wider transfixion is needed, more caudal to the previous attempt.
Once both of the ligatures have been placed, the cervix is crushed at their level with an intestinal clamp. Another clamp is then placed just above the first and the contents of the uterus are pushed back towards the horns; two other clamps are placed in the same way above the 2nd clamp. The 2nd and 3rd clamps are removed, thus leaving a secretion-free zone.
Sectioning the Cervix: Once both intestinal clamps have been placed, the anterior section of the cervix is performed; the cervix may be normal or pathological.
Normal Cervix: The cervix is simply sectioned with a scalpel between the two clamps.
Pathological Cervix: For pathological cervixes, the serosa is dissected just caudal to the clamp that is placed on the uterus; the serosa is then retracted caudally. The musculosa is then sectioned cranial to the intestinal clamp placed on the cervix; if the clamps have been placed correctly, no fluid should leak from the cut ends.
Dealing with the Stump
Small, Normal Cervix: The stump is simply replaced in the abdominal cavity. It is however advisable to suture it or bury it in a fold of omentum.
Pathological Cervix: The cut section of the musculosa, mucosa, is cauterised with an iodine-based solution, and then sutured in two phases:
- Septic Phase: For the septic phase, a simple continuous suture is made in the musculosa with polyglycolic acid.
- Aseptic Phase: The needle is changed and either a buried simple continuous suture is made with the serosa (sero-serous continuous suture), or the stump is enfolded in one of the broad ligaments, which is fixated with a suture in the bursa. The ligament will weld itself to the stump. Finally, the stump can be invaginated by burying it in the vagina, then placing a ligature a few centimetres behind the original section. However, invagination is practically impossible to perform in small dogs due to the small size of their genital tract. These suture procedures eliminate the risk of peritoneal infection, since the pathological secretions drain into the vagina.
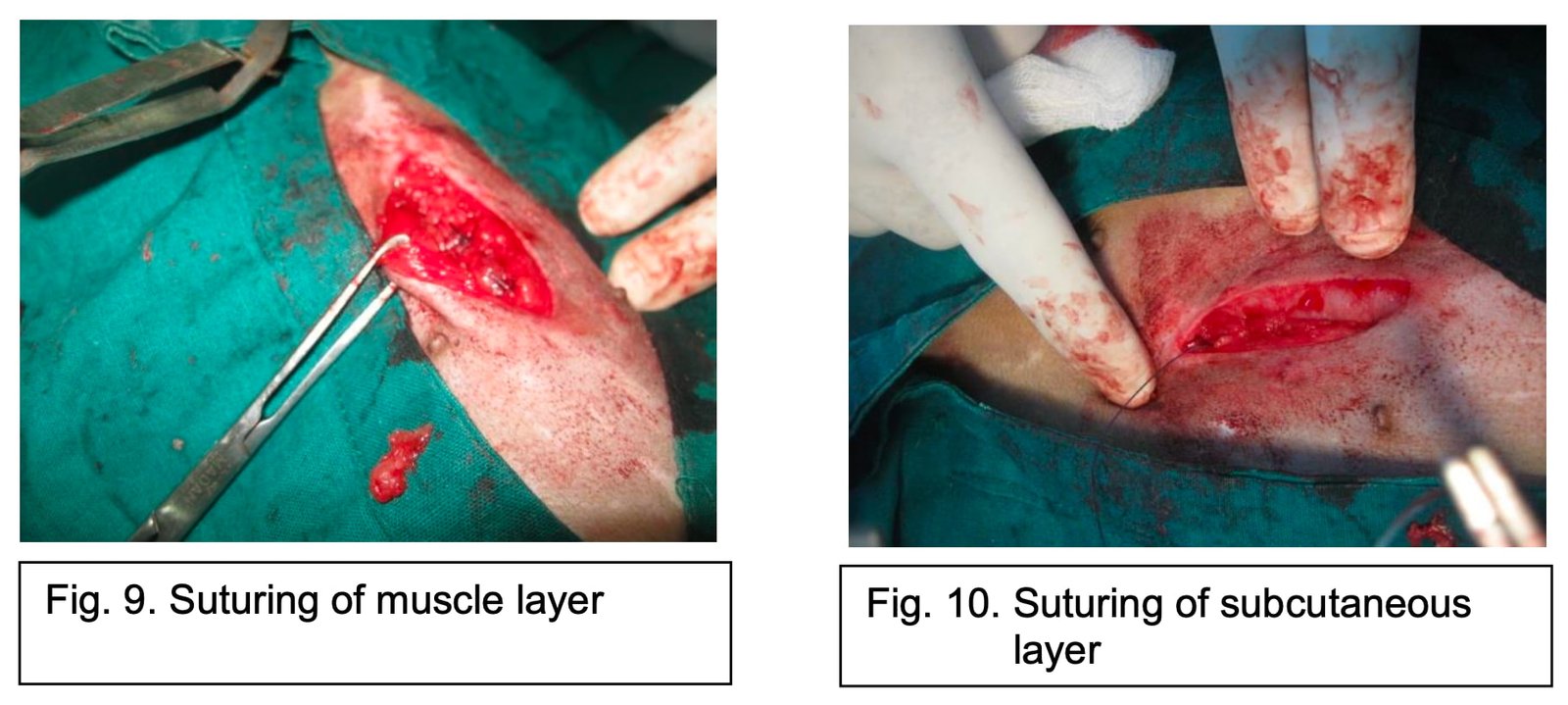
Suturing the Abdominal Wall and Skin: The sutured stump is returned to the abdominal cavity and the abdominal wall is closed using simple continous suture pattern with polyglycolic acid (No. 1-0/1) (Fig. 9). If the subcutaneous connective tissue is very abundant, a simple continuous subcutaneous suture is performed using polyglycolic acid (No. 1-0/1) (Fig. 10).
Finally, the skin is sutured using intradermal sutures using 1-0 polyglycolic acid (Fig. 11) or mattress sutures with non-resorbable suture materials such as silk. The wound is then disinfected with antiseptic solution and protected with a few swabs and an adhesive dressing.

Complications of Ovariohysterectomy
Ovariohysterectomy (OHE/OVH) and orchiectomy are two of the most commonly performed surgeries in companion animal practice. Techniques for accomplishing surgical sterilization may be by flank approach or by mid ventral approach. Complications do not differ much when OHE done by these two approaches.
Complications of Ovariohysterectomy includes hemorrhage, wound healing complications, ovarian remnant syndrome, stump pyometra, uterine stump abscess/granuloma formation, obstipation, ureteral trauma and urinary incontinence.
The list of complications of ovariohysterectomy (OHE) in dogs includes:
- Hemorrhage
- Wound Healing Complications
- Ovarian Remnant Syndrome (ORS)
- Stump Pyometra
- Ureteral Injury
1. Hemorrhage
Hemorrhage is the most common complication of ovario hysterectomy.
Diagnosis/Therapy
Detection of intra-abdominal haemorrhage can be challenging, as clinical signs following ovariohysterectomy (OHE) are often nonspecific. These may include delayed recovery from anaesthesia, pale mucous membranes, and tachycardia. In some cases, dogs with acute postoperative hemoperitoneum may leak large volumes of non-clotting, bloody fluid from the incision site—a finding that can be mistakenly attributed to bleeding from subcutaneous vessels.
Animals presenting with such signs should be evaluated for significant hemoperitoneum using ultrasound imaging and abdominocentesis. In the absence of ultrasound, abdominocentesis can be performed blindly using 20-gauge needles inserted at paramedian sites along the ventral abdomen, following strict aseptic technique. The presence of non-clotting intraperitoneal fluid with a packed cell volume (PCV) approximating or exceeding the animal’s peripheral PCV is diagnostic for intra-abdominal haemorrhage.
Based on findings from physical examination, ultrasonography, and haematological testing, the clinician must determine whether the haemorrhage can be managed conservatively (e.g., with abdominal bandaging and intravenous fluid therapy) or if surgical intervention is required for re-exploration and re-ligation of the pedicles.
Avoidance
Intraoperative hemorrhage during ovariohysterectomy is most commonly associated with rupture of the right ovarian pedicle during attempted release of the suspensory ligament. Occurrence of this complication has been attributed largely to rough tissue handling by novice surgeons and also due to insufficient knot-tying technique, a problem that is most often revealed when a surgeon-in-training attempts to ligate a large, fat-filled pedicle in a mature female dog.
In a training institution, avoidance of ovarian pedicle rupture is facilitated by encouraging ample abdominal exposure through incisions that extend from the umbilicus to the last mammary teat, allowing access to the right ovarian pedicle, which is located in the craniodorsal abdomen. Rather than strumming the suspensory ligament, grasping the cranial edge of the suspensory ligament between the thumb and index finger, sliding the thumb and finger down into the incision, and breaking the suspensory ligament with a twisting motion of the finger and thumb right at the point of attachment on the body wall will avoid bleeding. This technique allows for controlled rupture of the cranial edge of the suspensory ligament at a location that is distant from the origin of the vascular pedicle.
Ligation is performed using 3-clamp technique, with each ovarian pedicle being doubleligated and transfixed.
2. Wound Healing Complications
Development of wound complications has also been related to duration of surgery, with an increased incidence of postoperative swelling and wound infections occurring after surgeries that lasted longer than 90 minutes and in anesthetic episodes lasting longer than 120 minutes. Seroma formation along the ventral midline is also a quite common complication due to the dependent location of the wound, which facilitates collection of fluid.
This complication must be distinguished from the subcutaneous swelling that is associated with more serious abdominal wall dehiscence and herniation of the falciform fat or small intestine. Diagnosis of abdominal wall herniation is usually made by palpation of a defect in the abdominal closure in association with the appearance of a subcutaneous soft tissue mass effect. Unless self-induced trauma has occurred, the skin closure is typically intact and hernia repair can be performed on a semi elective basis.
Confirmation of the diagnosis can be made with plain radiography, which may show a defect in the ventral abdominal wall on lateral projections or by using abdominal ultrasound examination.
Avoidance
Abdominal wall dehiscence that occurs during the first 7 days after surgery is most commonly due to technical errors, including failure to incorporate the external rectus fascia, inappropriate suture size, or knot failure. Many of these technique errors can be avoided by use of proper surgical technique. Clearing of subcutaneous tissues from the external rectus fascia for approximately 1 cm on either side of the linea alba facilitates proper incorporation of the external rectus fascia during closure.
The linea may be closed in either a continuous or an interrupted appositional suture pattern, using monofilament, absorbable suture material. Due to the slow healing rate of abdominal wall fascial incisions, a suture with prolonged retention of tensile strength is recommended, such as PGA.
3. Ovarian Remnant Syndrome (ORS)
Ovarian remnant syndrome is a rare complication of OHE in dogs and cats. Residual ovarian tissue most commonly results from incomplete resection of the ovary during the initial surgery, maintaining functional status indefinitely. Diagnosis is typically suspected in dogs with a history of OHE that later develop clinical signs of proestrus or estrus, with most commonly reported signs including vaginal discharge, vulvar swelling, and behavioral changes. Confirmation of the diagnosis can be made using vaginal cytology, hormonal testing, abdominal ultrasound, and exploratory laparotomy.
Therapy
Surgical exploration and resection of retained ovarian tissue have led to resolution of clinical signs in all reported cases of ovarian remnant syndrome. It has been suggested that performing the exploratory surgery during a time of active proestrus, estrus, or diestrus can facilitate identification of ovarian tissue due to the presence of follicles, corpora leutea, and increased size of the ovarian vascular pedicle.
Retained ovarian tissue is typically noted to be located in close association with the fibrous tissue that marks the location of the original ovarian pedicle ligation and can be distinguished from surrounding adipose tissue by the darker coloration and firm character of ovarian tissue. Ovarian pedicle remnants are located caudal to the kidneys and are often in close association with the ureters. Thus, the surgeon must take great care in identifying the ureter prior to resecting the ovarian remnant.
Avoidance
The ovary can be very difficult to visualize, especially in dogs, due to the large amount of adipose tissue associated with the mesosalpinx in this species. As a result, a variety of strategies have been used to ensure complete removal of the ovary during OHE. First, adequate exposure is obtained in the initial midline abdominal incision so that the ovary can be completely exteriorized during clamp placement.
The suspensory ligament is ruptured or stretched to a degree that allows mobilization of the ovary so that there is adequate space to place two hemostatic clamps on the ovarian pedicle without encroaching on the ovary. Because visualization of the ovary is often obscured by fat in the mesosalpinx, digital palpation of the ovary is performed while placing the hemostatic clamps on the ovarian pedicle, making sure to place the clamps at least 1 cm proximal (or deep) to the ovary on the ovarian pedicle.
Ligatures are then placed proximal to the clamp, ensuring that the ovary will be completely resected when the pedicle is severed distal to the ligatures. As a final precaution, the ovary is examined directly for its complete removal before releasing the ovarian pedicle.
4. Stump Pyometra
A common misconception is that stump pyometra occurs as a result of incomplete resection of the uterine body. It is important to remember that the pathophysiology of stump pyometra is identical to that of classic canine pyometra, involving repeated exposure of the uterus to progesterone from either an ovarian remnant or, much more rarely, the therapeutic administration of exogenous progestogens. Thus, stump pyometra is not caused by retained uterine tissue; it is actually a rarely reported complication of ovarian remnant syndrome.
A key diagnostic finding is the presence of a fluid-filled uterine stump on abdominal ultrasound in a dog that has a history of previous OHE. Further examination by a skilled operator may allow detection of the retained ovarian tissue that is invariably the cause of this complication.
Therapy
Resolution of stump pyometra is achieved by resection of the uterine stump at the level of the cervix. A caudal midline celiotomy is performed and the uterine stump is located by retroflexing the urinary bladder and identifying the uterus between dorsal to the urinary bladder and ventral to the colon.
The uterine stump is double-ligated and transfixed with absorbable monofilament suture, just cranial to the cervix. The uterine stump is flushed copiously with sterile 0.9% NaCl. If there is remaining concern about ongoing contamination, the omentum may be sutured to the end of the uterine stump to form a fibrin seal while providing physiologic drainage of the area.
Avoidance
Uterine stump pyometra is one manifestation of ovarian remnant syndrome. As a result, avoidance strategies are identical to those of ovarian remnant syndrome.
5. Ureteral Injury
The ureters travel through the retroperitoneal space caudal to the kidney and are crossed by the gonadal arteries, where they can be inadvertently traumatized or ligated during OHE. Diagnosis of ureteral injury is typically obtained using a combination of imaging modalities since no single modality is ideal for all situations.
Intravenous urography is most useful in detecting the location of upper urinary tract rupture in animals with normal renal function, but abdominal ultrasound is more adept at imaging the urinary tract in cases of chronic obstruction, when deteriorated renal function can limit the detectable contrast that reaches the collecting system.
Therapy
Ureteral repair is technically demanding and, in smaller animals, requires the use of microsurgical instruments and an operating microscope. As such, animals with suspected ureteral injury after OHE should be referred to a surgeon with the equipment and experience required to successfully perform these surgeries.
Avoidance
Ureteral injury is avoided by constantly being aware of the anatomic location and proximity of the ureter to the operative site. Inadvertent injury to the ureter can occur if a surgeon grasps to retrieve a dropped ovarian pedicle that has retracted into the retroperitoneal fat caudal to the kidney.
Inadvertent incorporation of the ureters in the uterine stump ligation is facilitated by complete preoperative emptying of the urinary bladder during preparation of the skin. The empty bladder moves caudally in the abdomen, pulling the ureters away from the region of uterine stump ligation and improving visualization during ligation.