TABLE OF CONTENTS
Caesarean Section (C-section) in Veterinary Obstetrics
A caesarean section (C-section) is a surgical procedure performed to deliver a fetus when natural delivery is not possible or safe for the dam or her offspring.
Caesarean (Cesarean) section is the delivery of a fetus, usually at parturition, by laparohysterectomy.
Caesarean section (C-section) in animals is performed when mutation, forced extraction, and fetotomy are deemed inadequate or too difficult to relieve the present dystocia, or when it is desired that the fetus be delivered alive.
Indications of Caesarean Section
- Fetal Oversize: Fetal oversize may be due to fetopelvic disproportion, physical immaturity of the dam, absolute oversize of the fetus in certain breeds of cattle, fetal anasarca, fetal emphysema, and post-maturity.
- Incomplete Cervical Dilatation: This may be associated with secondary uterine inertia with advanced involution of the cervix, cervical inertia, etc.
- Irreducible Uterine Torsion: Torsion of the uterus in cattle constitutes a major indication for caesarean section, either because the torsion is irreducible or because the cervix remains inadequately dilated for vaginal delivery after detorsion.
- Fetal Deformities: Cattle, more than most species, are susceptible to gross structural developmental abnormalities. Examples include schistosomus reflexus, achondroplasia or bulldog calf deformity, anasarca or fetal dropsy, muscle contracture monster, arthrogryposis associated with torticollis and kyphosis, perosomus elumbis, and conjoined twins.
- Faulty Fetal Disposition: Provided that the cervix is fully dilated and remains so, most early cases of fetal malpresentation and malposture can be corrected manually or relieved by simple fetotomy. However, the loss of fetal fluids followed by the loss of uterine contractions often makes the manipulations difficult and time-consuming, increasing the risk of uterine rupture. In protracted cases, constriction of the cervix may prevent vaginal correction of the dystocia, and the fetus is then likely to become emphysematous.
- Fetal Emphysema: This is a frequent complication of delayed dystocia in cattle and, irrespective of the primary cause of dystocia, is often the immediate indication for caesarean section.
Miscellaneous indications: The natural termination of a pathologically prolonged pregnancy may be associated with the absence of normal parturient changes in the vagina and vulva, necessitating a caesarean section.
- Abortion in late pregnancy sometimes requires caesarean section for several reasons, such as incomplete birth canal dilatation, cervical constriction, fetal deformity, malpresentation, malposture, or emphysema.
- Fetal mummification and hydrops uteri may be treated by inducing parturition, but a cesarean section may be necessary if induction fails or if the birth canal is insufficiently dilated for vaginal delivery.
- Laparotomy is essential in cases of uterine rupture.
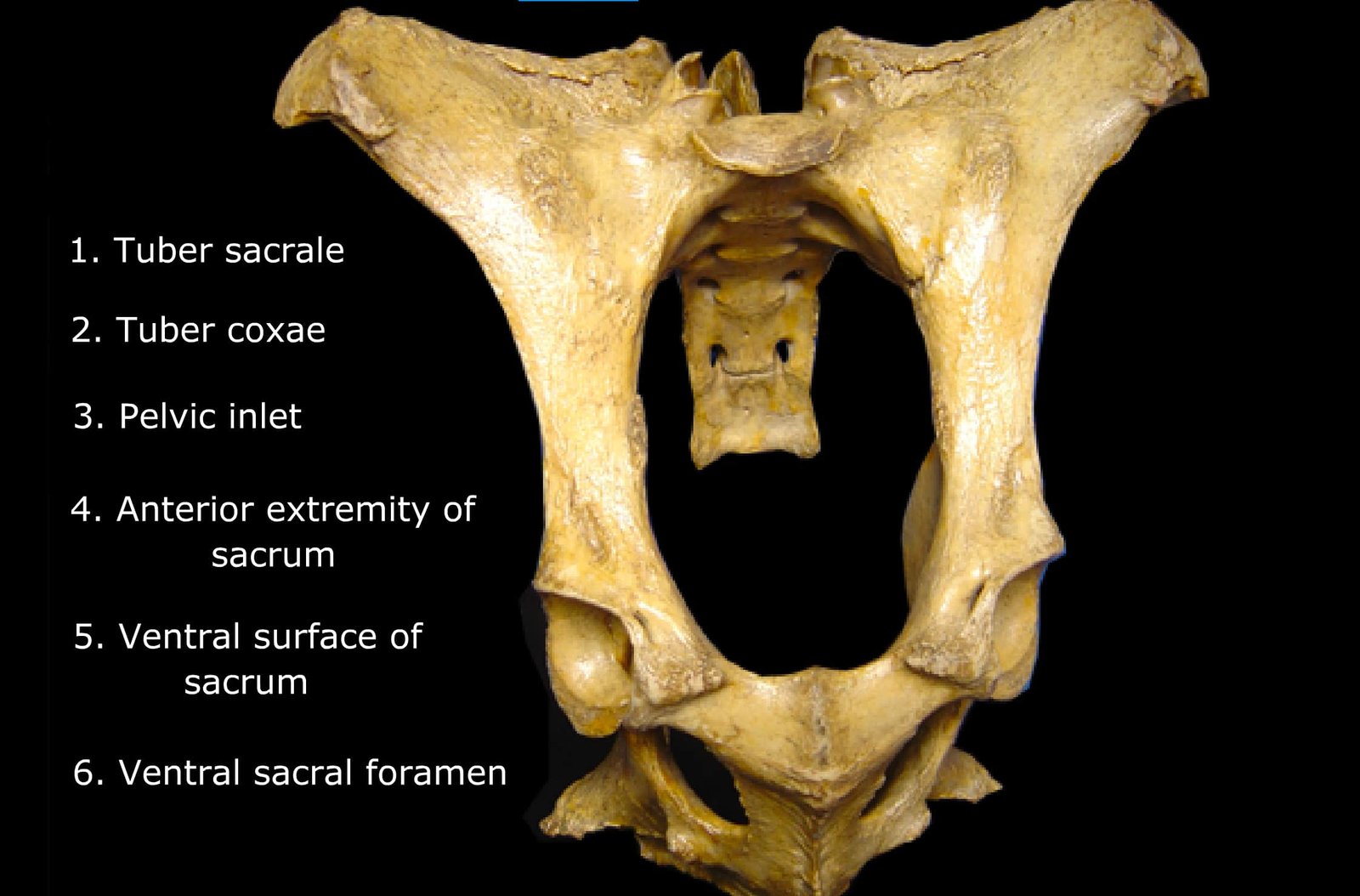
Selection of the Operative Site
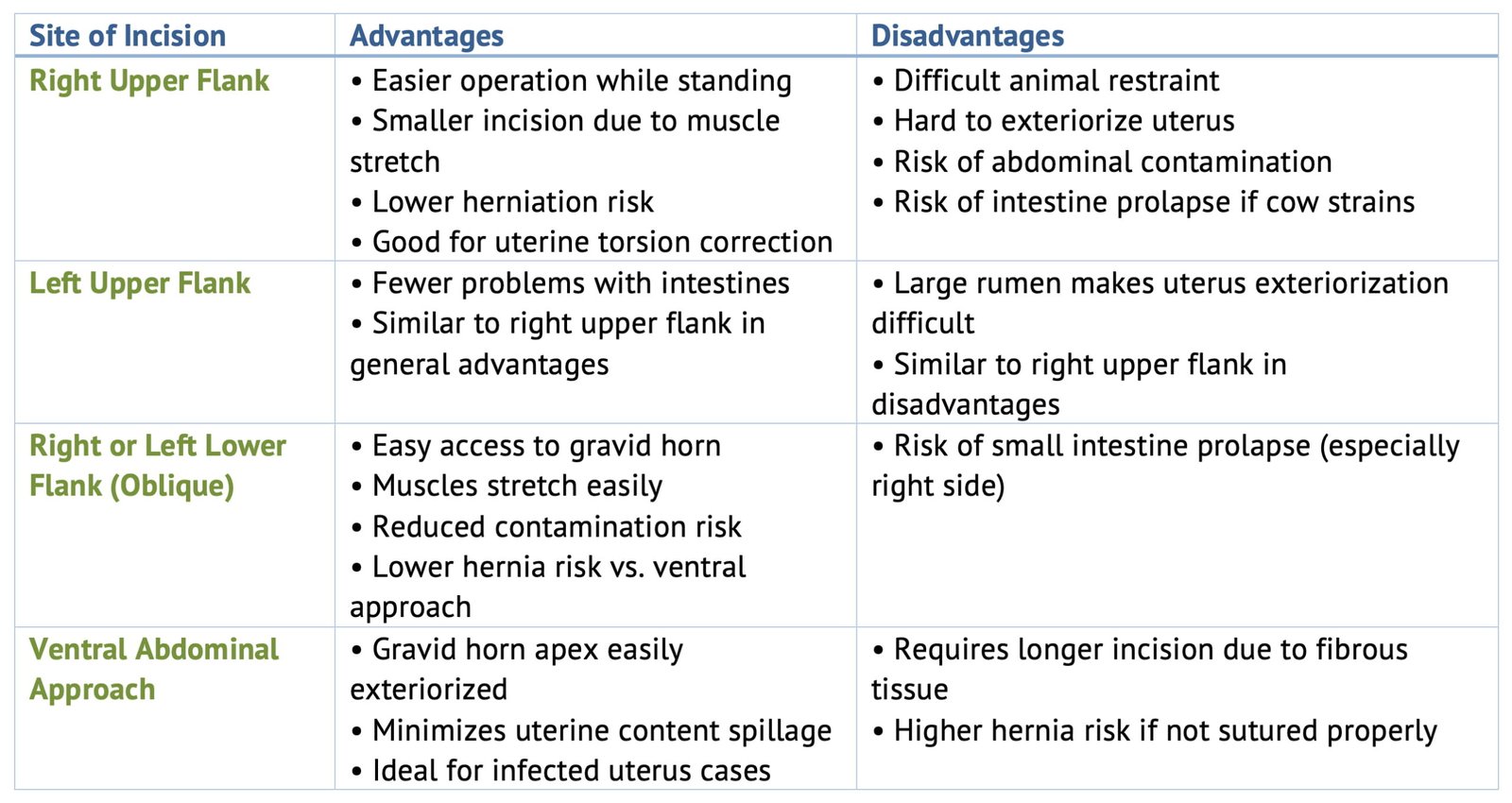
Right Upper Flank
Advantages
- The right upper flank site makes the operation easier and allows it to be performed while the animal is standing.
- The incision can be smaller because the muscle tissues stretch into a circular shape when the fetus is removed.
- The chances of herniation are less.
- The right flank approach may be preferred when torsion of the uterus is present, as the standing position assists in correcting the torsion.
Disadvantages
- The cow may be more difficult to restrain and control.
- It is difficult to bring the uterus to the incision, and abdominal contamination with uterine contents is nearly unavoidable.
- If, during the operation, the incision is extended too far ventrally, it becomes difficult to hold the small intestines within the abdomen.
- If the cow strains, coughs, or struggles, an armful of intestines may be expelled through the laparotomy incision, and occasionally, the cow may put her foot through them.
Left Upper Flank
Intestines are not present to pose a problem in the left upper flank site of operation. However, a large, full rumen may make it quite difficult to bring the uterus from the right side of the abdominal cavity to the left. Other advantages and disadvantages are similar to those of the right upper flank site.
Right or Left Lower Flank Oblique Abdominal Incision
Advantages
- Easy access to the gravid horn.
- Muscles in this region stretch easily.
- It is easier to prevent contamination at the abdominal cavity by uterine fluid.
- There is less possibility that hernia will develop than when the incision is on the ventral aspect of the abdomen.
Disadvantages
The disadvantage of this site on the right side is that it is necessary to control the small intestines during the operation to prevent them from prolapsing.
Ventral Abdominal Approach
In all ventral abdominal incisions, the incision starts at or slightly lateral to the fore udder and extends forward as far as necessary, usually 12–14 inches.
Advantages
The apex or ventral portion of the gravid horn can be brought to and outside the incision, thereby preventing uterine contents being released into the abdominal cavity. This is a great advantage in cases in which uterus is infected.
Disadvantages
The abdominal wall at this site is composed of largely fibrous tissue tunics and will not stretch and does muscle tissue. Thus the incision must be longer than in the flank. If the proper suture material and technique are not employed herniation is more common.
Anaesthesia for Caesarean Section
- Local infiltration or inverted ‘L’ block
- Paravertebral nerve block (Rarely used)
- Epidural anaesthesia (To avoid straining)
- Sedation with xylazine
Operative Technique
- After preparing the surgical site, local infiltration with an anaesthetic agent is done.
- Mostly, a left or right lower flank approach for caesarean is performed.
- An incision of about 10–12 inches is made on the skin.
- Then the external oblique, internal oblique, and transverse abdominus muscles are incised with blunt dissection.
- The peritoneum is cut with a knife and incised with scissors.
- Omentum may be pushed cranially or may be incised.
- The gravid horn containing the fetus is identified. The incision is made on the greater curvature of the uterus by avoiding placentomes.
- The fetus may be removed by caudal and lateral traction. If the fetus is alive, resuscitation of the fetus may be carried out.
- After a live fetus has been removed, the fetal membranes are left in the uterus.
- If the fetus is dead, the fetal membranes are removed manually if they drop away readily. Otherwise, they are left within the uterus. Some of the fetal membranes may be trimmed away with scissors so that they do not interfere with the suturing of the uterus.
- Because of the high incidence of uterine infection and retained afterbirth following caesarean section, it is advisable to place 2–4 gm of oxytetracycline in the uterine cavity, whether or not the fetal membranes are removed.
- The uterine incision is closed with a double row of Lembert or cushion sutures of No. 2 or 3 chromic catgut.
- If the caesarean is performed for uterine torsion, and if the torsion was not corrected before the fetus was removed, it should be corrected after uterine closure is completed.
- The uterus should always be examined for the presence of twins, although they are rarely encountered in cases of caesarean section.
- The omentum is sutured, if incised, with No. 2 chromic catgut.
- The peritoneum is sutured with a continuous suture using No. 2 chromic catgut.
- Abdominal muscles are sutured with No. 2 or No. 3 chromic catgut using continuous lock sutures or horizontal interrupted mattress sutures.
- The skin incision is closed with simple interrupted, cross mattress, or horizontal mattress sutures using nylon or cotton thread, and skin sutures are usually removed in 7 to 10 days.
- Postoperative care with intravenous fluids, parenteral antibiotics, antihistaminics, and analgesics is given.
- After the operation, 30 to 50 units of oxytocin and 300–450 ml of calcium borogluconate may be administered to aid uterine involution.
Post Operative Complications
Immediate Complications
- Maternal death due to shock, secondary to exhaustion, toxaemia, haemorrhage and excessive manipulation of abdominal viscera or sudden release of intra abdominal pressure as in hydrops.
- Retained fetal membranes
- Metritis
After Few Days
- Wound break down
- Suture abscess
- Seroma in the incision site
- Subcutaneous emphysema
- Peritonitis and death
Later Stages
- Hernia
- Adhesions
- Infertility