TABLE OF CONTENTS
Sesamoiditis in horses
Sesamoiditis in horses is observed frequently in racing horses and hunters and jumpers between 2 and 5 years of age.
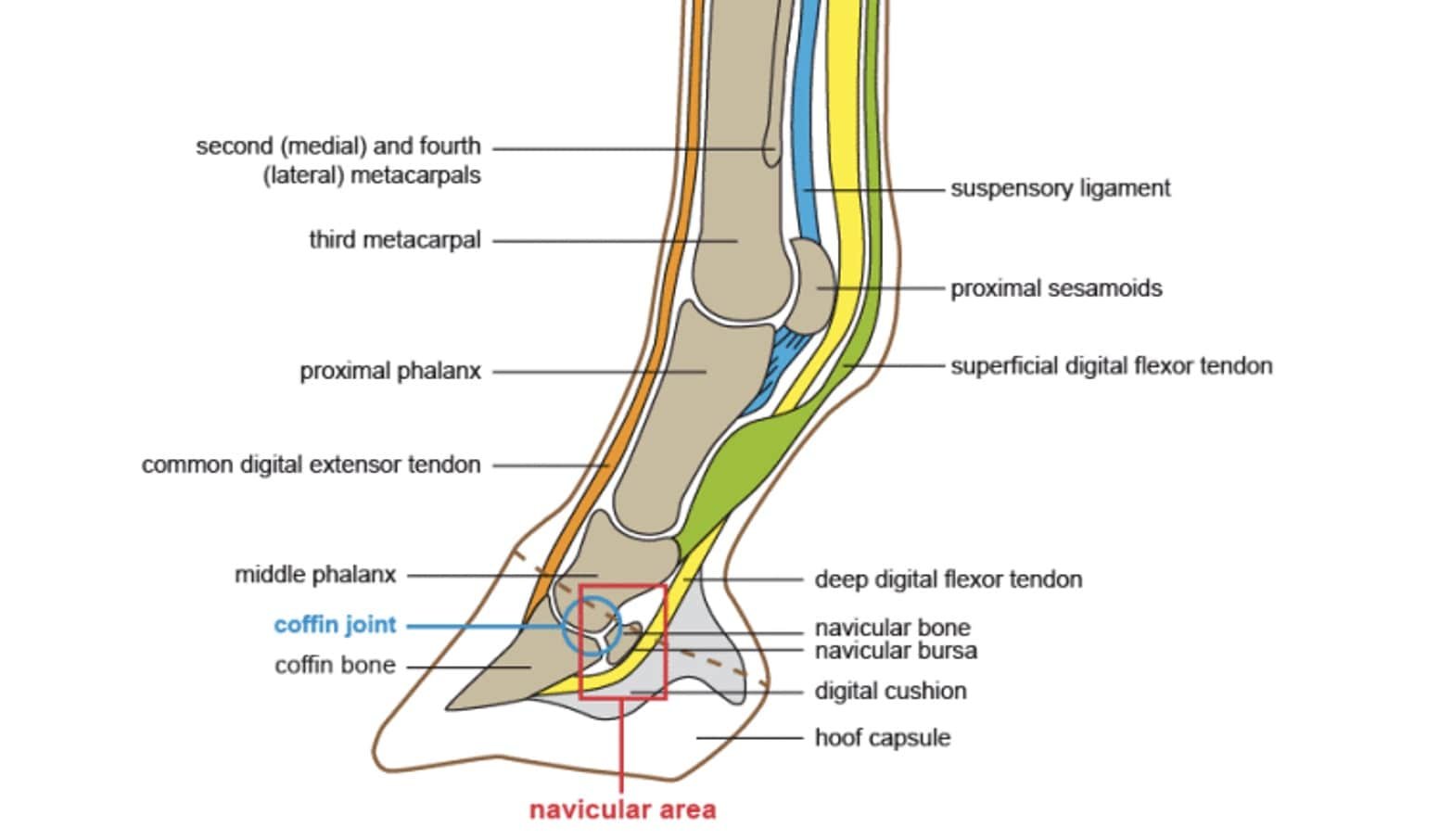
The sesamoid bones are maintained in position by the branches of the suspensory ligament proximally and by a number of sesamoidean ligaments distally. Because of the great stress placed on the fetlock during fast exercise, the abaxial portion of the proximal sesamoid bones is susceptible to stress-related injury. Sesamoiditis is a clinically distinctive condition; however, it is poorly characterized pathologically.
The Sesamoiditis condition is characterized by pain associated with the proximal sesamoid bones and insertions of the suspensory ligament that result in lameness. The pain is thought to result from inflammation at the interface of the suspensory ligament and distal sesamoidean ligaments with the proximal sesamoid bone.
Primary disease of the suspensory ligament or distal sesamoidean ligament can also accompany this condition.
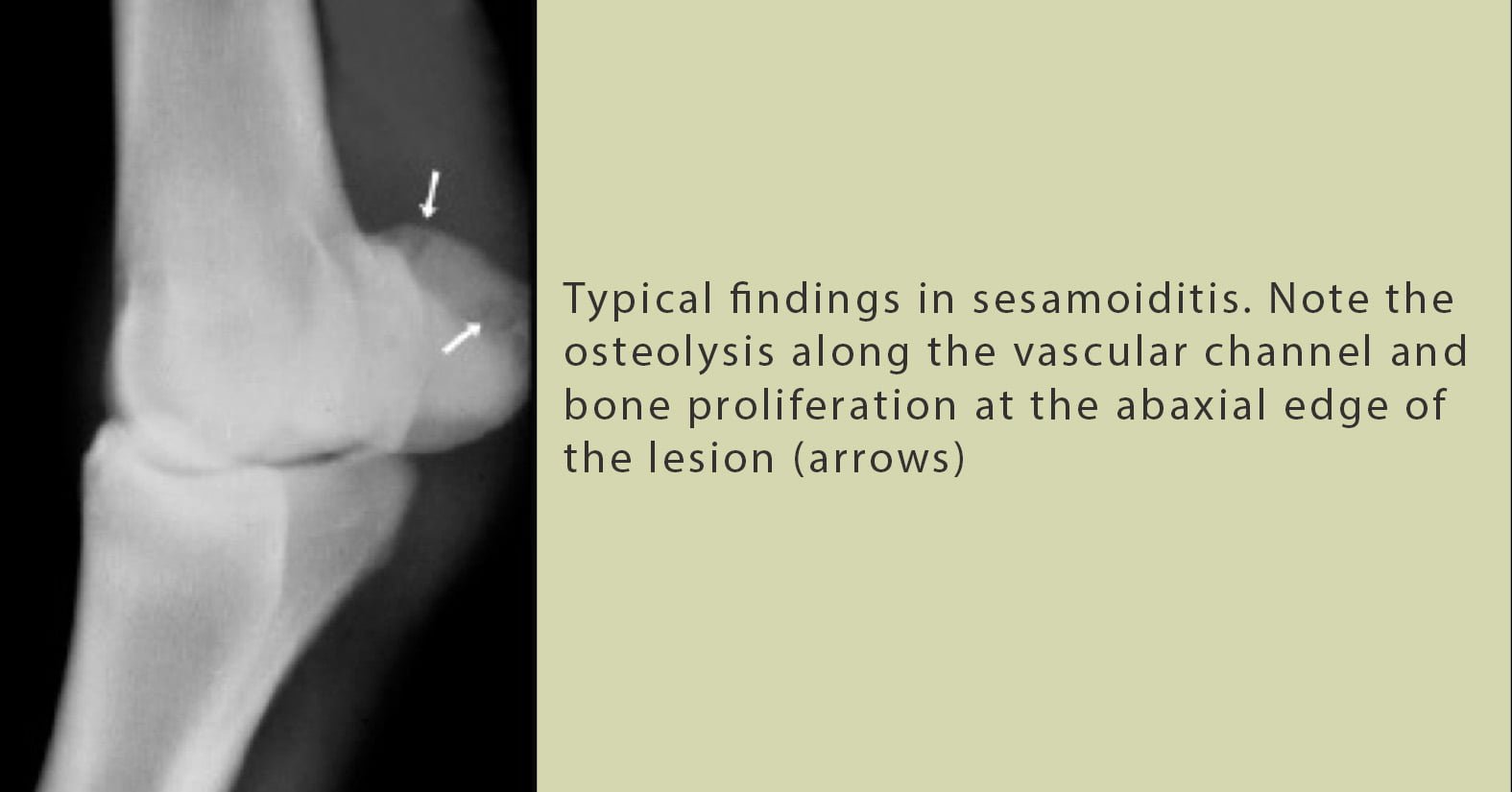
Radiographic evidence of sesamoiditis involves periarticular osteophytes, entheseophytes, focal osteolysis, and enlarged vascular channels (or linear defects in the abaxial margin of the proximal sesamoid bones).
Etiology
- Unusual strain to fetlock region
- Common in race horses, hunters and jumpers
The recommended treatment is enforced rest and symptomatic treatment to combat inflammation and soreness. The insertion of the suspensory ligaments should also be carefully evaluated by ultrasonography for concurrent lesions.
Clinical Signs
- Similar to sesamoid fractures
- Minimal swelling and heat observed may felt over the abaxial surface of the sesamoid bone during early stages of sesamoiditis
- As the disease progresses, a visible enlargement of the soft tissues overlying the palmar surface of the fetlock can be seen as fibrosis of the injured suspensory ligament becomes apparent.
- On palpation, pain withdrawal can usually be elicited by placing pressure over the abaxial surfaces of the sesamoid bone.
- In more advanced cases, pain may be elicited by applying pressure over the branches of the suspensory ligament and possibly the distal sesamoidean ligament as well.
- Flexion of the fetlock is also painful.
- Different degree of lameness during exercise
- On close observation, a reduction in extension of the fetlock is noticed, and a fetlock flexion test usually exacerbates the lameness
- Perineural and/or intrasynovial anesthesia is used infrequently to diagnose this condition. Horses respond to a distal metacarpal nerve block, but not to an intra-articular fetlock block, locating the lameness to the periarticular structures.
Diagnosis
- Radiography
- Ultrasound examination
- Nucear scintigraphy
Treatment
- If heat, pain, and swelling are detected at the bone or suspensory insertion, then efforts should be made to reduce the inflammation.
- Alternating cold and hot packs, as well as antiphlogistic packs, should be used.
- Rest from performance until soundness at the trot is achieved followed by slow convalescent exercise allows the bone to continue to remodel and strengthen. Importantly, the exercise must be kept below the level that would reinjure the bone.
- Similar to other suspensory ligament injuries, convalescence is long (6 to 8 months) and injury often recurs when horses return to full work.
- In chronic stages, firing, and blistering have been used but with only limited success. X-ray and gamma-ray radiation, laser heat application, shock wave therapy, and a balanced mineral diet are considered by some to be valuable therapy in this condition, as well as in the treatment of calcification in the suspensory ligament.
Prognosis
The prognosis of Sesamoiditis in horses for return to full athletic performance is guarded to unfavourable, depending upon the amount of periosteal reaction and new bone growth that occurs on the sesamoid bones and the extent of injury to the suspensory ligament and the distal sesamoidean ligaments.