TABLE OF CONTENTS
Reproductive Abnormalities in Mares (Female Horses)
Reproductive abnormalities in mares (female horses) is diagnosed by history, physical examination, clinical examination etc.
History
As a rule, there is less recorded history available about mares than cows, and the information which might be obtained is less complete. If possible, information should be acquired with regard to the following:
- Age of the animal.
- Duration of the present ownership.
- Previous pregnancies and foaling, if any.
- Date of the last foaling and the rate of growth and development of the foal.
- History of any infections.
- The month of commencement of the breeding season as well as its length.
- Intensity of estrus, the length of the estrus period and the length and regularity of the estrous cycle.
- The client should be asked about the method employed for observing heat.

Physical Examination
Visual Examination
Conditions that alter the general conformation and the external appearance of the cow are simply not encountered in the mare. Changes in the appearance of the “tailhead” are not as apparent in the mare.
Relaxation of the pelvic diaphragm and vulva associated with gestation is observed during the last 2 to 5 days of pregnancy, and then not in all animals.
Copious discharge of estrus mucus is seldom observed in the mare. Thus, information suggesting physiological events cannot be obtained by visual inspection.
Significant information, however, is gained from observing conformation changes involving:
- External genital organs.
- Abnormal vaginal discharge.
- Hoof and leg infirmities such as a rotated third phalanx following acute laminitis that may make a mare reluctant to stand for breeding or may make her unfit to carry a pregnancy to term.
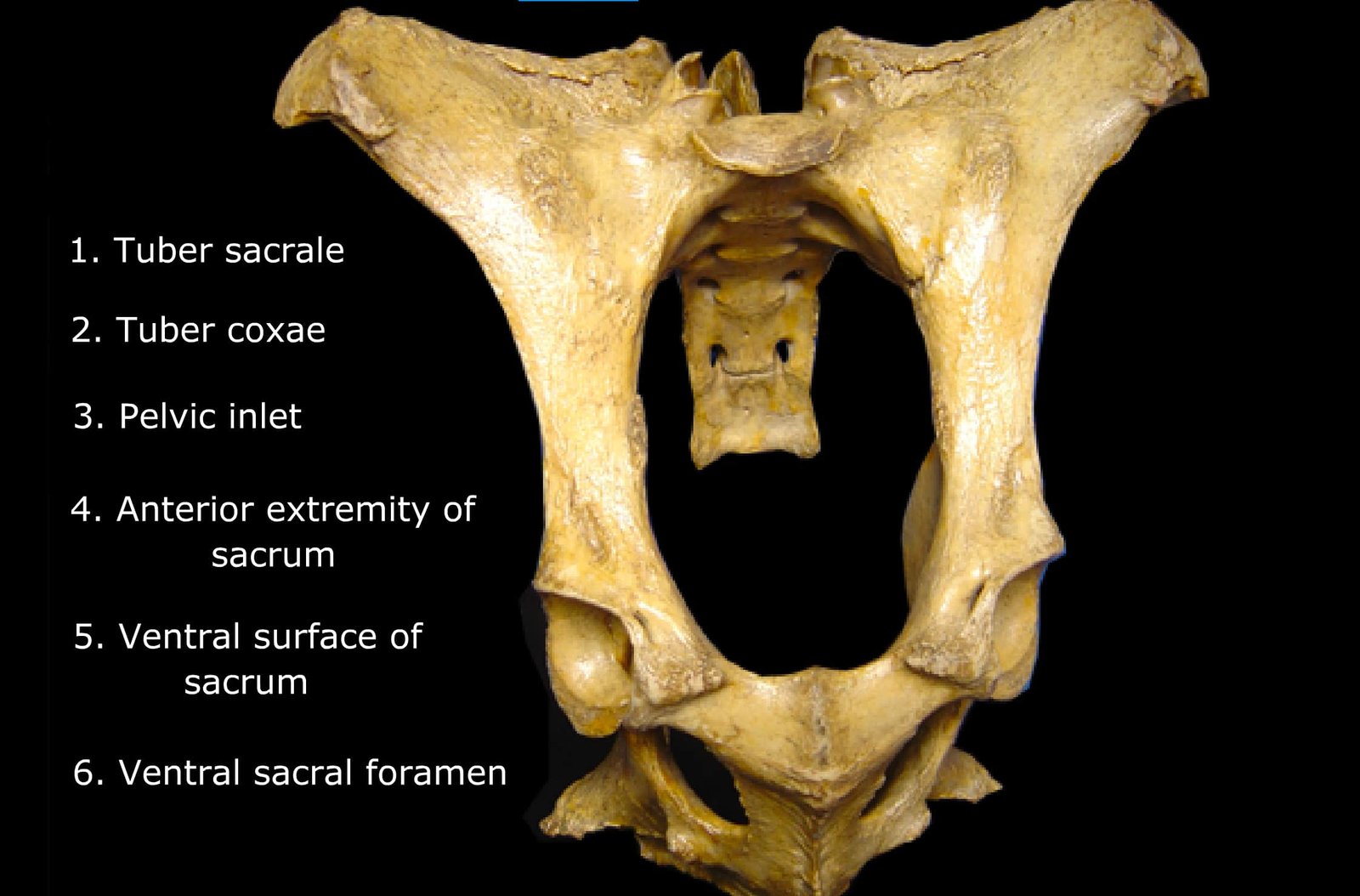
- Pelvic injuries or abnormalities that may predispose a mare to dystocia.
- Small stature.
- Hirsutism associated with a pituitary tumor may be the cause of a mare‘s unseasonal anestrus.
- Hypertrophic pulmonary osteopathy has been associated with certain types of ovarian tumors in mares.
Examination of Genitalia
After completing the general physical examination, a detailed evaluation of the reproductive organs should be undertaken with the tail wrapped in gauze and tied out of the way.
Mammary glands should be examined and palpated for signs of mastitis, abscessation, neoplasia or injury.
Vulva should be examined for conformation, apposition, tone and evidence of discharges.
Mal-apposition of the vulvar lips or poor vulvar conformation may lead to pneumovagina and fecal contamination of the vaginal vault.
Examination of the vulvar area should continue with the examination of the clitoral fossa and clitoris that harbors the contagious equine metritis organism Hemophilus equigenitalis.
The examination then continues with either rectal or vaginal palpation.
Examination Findings

Pneumovagina
Pneumovagina or “windsucker” condition is the most frequent conformation change observed in mares.
In normal mares the long axis of the vulva occupies an almost vertical position. In pneumovagina it forms an acute angle with the horizontal plane. In extreme cases the vulva might be found in an almost horizontal position.
The vulvar lips are relaxed, resulting in partial exposure of the vestibulum and clitoris. Scar tissue and consequent deformation of the vulva lips are frequently observed in mares which have experienced dystocia and lacerations.
The anus is sunken and enhances the appearance of a more or less horizontally directed vulva. The relaxed vulva and its position facilitate contamination of the vagina with fecal material.
The relaxation permits aspiration of air into the vagina and also into the uterus, especially during estrus thus allowing saprophytic and pathogenic bacteria to gain entrance into the genital tract. Treatment should be directed at correcting the cause of pneumovagina, and concurrently treating the resulting acute endometritis. The former can be done surgically by Caslick‘s operation.
Almost all animals with pneumovagina are infertile and show signs of genital infection.
Rectovaginal Fistula
The trauma which results in rectovaginal fistula affects the perineum, vulva, vestibule and rectum. Localized internal fistulas are rare.
The lesions are easy to see, and the diagnosis of either type of fistula does not present any difficulties. This abnormality leads to contamination and consequent infection of the genital tract.
Abnormal Development of the Vulva
The vulva might be too small when compared with general body size.
Asymmetry of the vulva and overlapping of vulvar lips are abnormalities that result in improper closure of the vestibule and permit aspiration of air.
Discharge from the Vulva
During estrus the vulva is moist, but the copious discharge which is a sign of estrus in the cow is not present.
The very viscid discharge present in practically all cows in advanced pregnancies is absent in the mare.
Lochia, the grayish red discharge in the postparturient animal, appears in much lesser amounts and only for a few days in the postparturient mare.
Postestrual hemorrhage is not seen in the mare. The appearance of an abnormal discharge is, however, significant.
Abnormal discharges include haemorrhagic and purulent discharge.
Haemorrhagic Discharge
Bloody discharge from the vulva is always serious. In the recently serviced mare, it indicates service injuries.
Bloody discharge from a pregnant animal practically always indicates threatened or completed abortion.
Purulent Discharge
Purulent material in the vaginal discharge may be observed directly, or noticed as crusts on the thighs and a loss of hair between the thighs if the exudates has been discharging for a longer period of time.
Indicates the presence of inflammation in the genital or in the urinary tract, especially in the bladder.
Determination of the site of inflammation requires performing a vaginal examination and occasionally doing a rectal examination and urine analysis.
Vaginal Examination
The vaginal speculum or vaginoscope is more frequently used for vaginal examination in the mare than in the cow and is always indicated whenever an abnormal discharge has been observed.
Preparation
- Vulva and perineum are thoroughly cleaned.
- The tail is wrapped and tied out of the way.
- The area is disinfected using a mild surgical scrub.
- Caution is taken to prevent forcing fluid through the vulvar cleft into the vagina.
Examination
After drying the area the vulvar lips are separated and a sterile vaginal speculum, either tubular or the three-pronged Caslick speculum, is introduced into the vestibular area.
With the aid of a light, the speculum is used to examine:
- the cervical os for color and tone as soon as possible, since changes occur as cool air enters through the speculum.
- the vaginal wall for color, evidence of congestion or inflammation, tumors, lacerations and scars.
- the vaginal floor for evidence of exudates or fluid accumulation or injury.
- the dorsum of the vagina for evidence of injury or fistulation into the rectum.
Endometrial cultures can be obtained during speculum examination.
Physiological Findings During Vaginal Examination
Estrous cycle
Diestrum
- In the luteal phase vaginal mucosa is pale pink and rather dry.
- Speculum examination results in influx of air and ballooning of the vagina thus favouring visibility. However, exposure to air causes the mucosa to become congested and hence, the color of the mucosa should be noted immediately after insertion of the speculum.
- Secretion is absent.
Estrum
- Vaginal mucosa appears deep pink and glistening with a small amount of clear secretion on the floor of the anterior vagina
- The external os is relaxed and lies limp on the floor of the vagina but is, however, extremely sensitive to touch and responds quickly by becoming erect.
- The appearance of the cervix is greatly helpful in determining whether a mare is in estrus or not. The erect cervical os during the luteal phase has been described as a “rosebud,” whereas the relaxed external os during estrus has been described as “wilted rose.”
Pregnancy
- The vaginal mucosa appears dull, anemic, rough and extremely dry, and insertion of the speculum might be difficult.
- The external os is more or less relaxed and covered with a sticky, grayish secretion.
- The stickly mucus sticks to the vaginoscope and to the vaginal mucosa and resembles rubbery glue during manual examination of the vagina.
- These findings are encountered in diestrus mares also.
Abnormalities Detected During Vaginal Examination
Persistent hymen
- Easily diagnosed during the process of insertion of the speculum.
- Septum may be partial, and might be brushed aside during introduction of the speculum.
- If complete, it might lead to a condition resembling white heifer disease in cattle. This is more pronounced in maiden mares which have experienced estrus.
- The cervical and vaginal secretion produced during estrus accumulate anterior to the obstruction formed by the persistent hymen and cause distention of the vagina.
- Prolapse of the vagina and marked straining are common observed.
Inflammation of the vagina and cervix
- Recognized by the presence of purulent exudates on the floor of the anterior vagina.
- The cervix is open and often discharges purulent material during vaginal examination.
- The mucosa of the external os of the cervix and the vagina has an unhealthy red appearance.
- The observations described above, however, always accompany pneumovagina.
Scars, abrasions, ulcers and other defects of mucosa of the vagina
- Observed as complications after service and parturition injuries.
- Diagnosis, as a rule, is easy.
Retention of urine in the anterior vagina
- The history is that of an intermittent discharge of grayish material.
- Vaginal examination reveals vaginitis and cervicitis which is secondary, since the fluid retained in the anterior vagina is primarily urine with admixture of epithelial debris from the mucosa.
- The downward and forward slope of the vaginal floor which might be the primary cause of the condition.
Rectal Examination
Rectal examination is done to rule out pregnancy. If the mare is pregnant, the procedures that follow will be altered.
Due to the friable nature of mare‘s rectum cre is taken when conducting a rectal examination.
A well lubricated, gloved arm and hand is introduced one finger at a time through the anal sphincter into the rectum. With the fingers held together, the cupped hand should clean out the feces as far cranial as possible prior to searching for the reproductive tract.
One may locate the ovary first by reaching up into the sublumbar area ventral to the fourth or fifth lumbar vertebrae or the uterus first.
Examination for Pregnancy
- Pregnancy examination in mares should precede all other examinations and should form the first and basic step of the approach to any form of infertility problem.
- The earliest time during the gestation period when the laboratory tests for pregnancy are reliable is 60 to 80 days after conception. i.e., between the third and fourth expected estrous periods after service.
- Pregnancy diagnosis might be made by rectal examination as early as 30 to 35 days of pregnancy, thus providing ample time for treatment, if indicated, and rebreeding a few days later on the second expected estrus after service.
Normal Changes in Reproductive Tract
- Unlike seen in the cow, no dramatic and consistent changes in uterus are observed in the mare.
- During diestrus and proestrus, certain mares have a well defined, slightly contracted uterus.
- During the estrus period, the uterus appears edematous and firm. This consistency persists until ovulation, after which the uterus becomes limp and flaccid.
Seasonal Changes
Cystic Changes
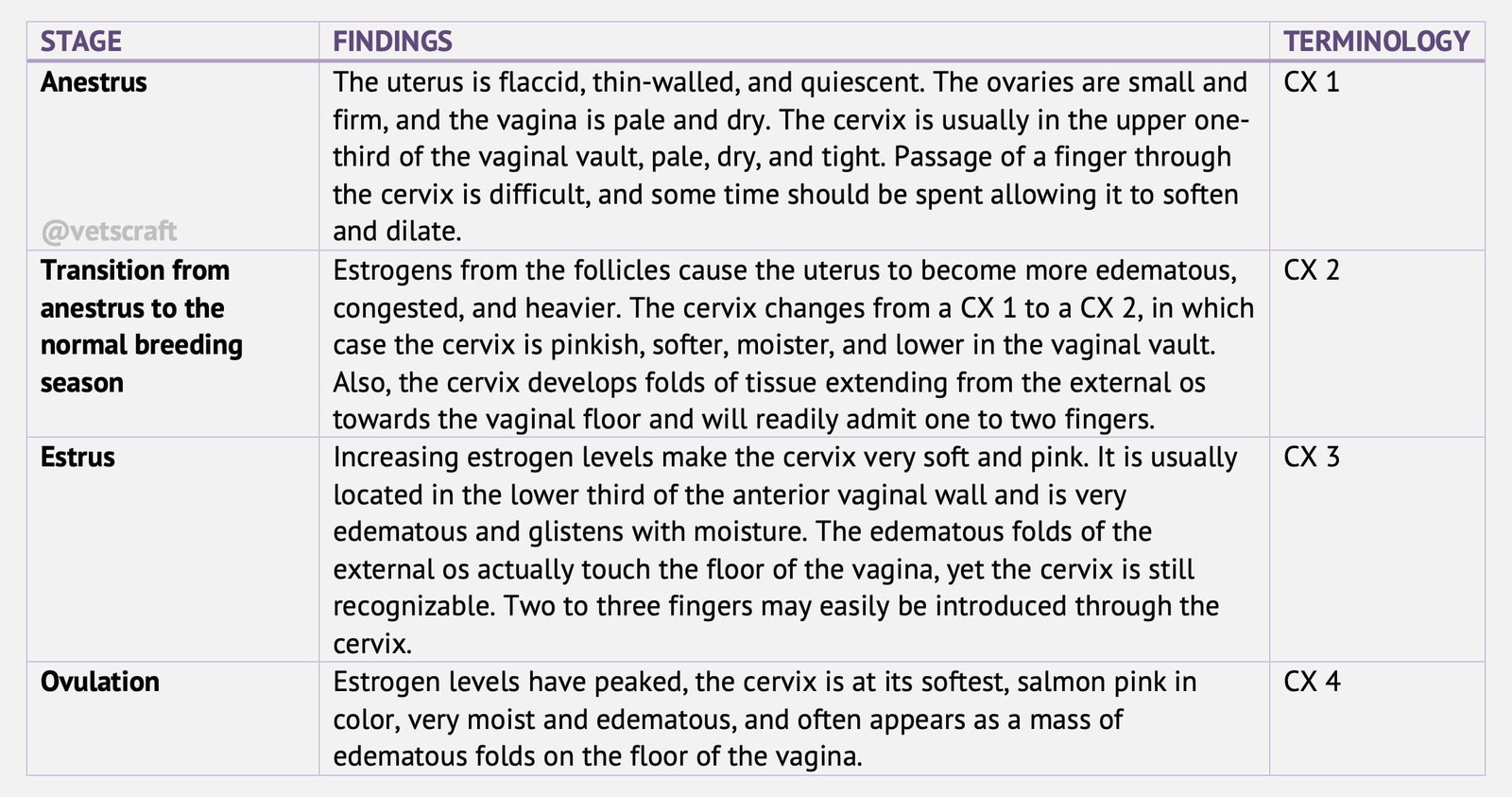
- Occasionally, a small pool of clear, serous mucus may be seen just caudal to the external os of the cervix. At this time, with stimulation, the cervix may dilate completely and readily allow the passage of the entire hand into the uterus.
- Another normal cervical condition that may be encountered in pregnancy is that of a “capped cervix” where the cervical appearance is similar to a CX 1 but in this case the external os is not visible because of a cervical plug and the appearance that one of the cervical folds has covered and sealed off the end of the cervix.
- After ovulation and during diestrus the uterus becomes less edematous, less congested and more tonic. It is easily identifiable as a firm tubular structure.
- The early pregnant uterus is also tonic and can be differentiated from the diestrus uterus by an amniotic vesicle bulge after about 20 to 25 days of pregnancy.
Post Parturient Involution of the Uterus
- Involution of the uterus after normal foaling is extremely rapid. Regression in size is almost completed at the 1st day of “foal heat”.
- The relatively low conception rate observed from services on the “foal heat” appear to indicate that the involution of the endometrium is not completed at this time in all mares.
Abnormalities Involving Uterus
Uterine abnormalities can be subdivided into:
- Abnormalities associated with a uniformaly enlarged uterus.
- Abnormalities associated with discrete abnormalities within the uterus.
- Parauterine abnormalities.
Uniformaly Enlarged Uterus
Must be differentiated from pregnancy and a postpartum uterus. Involution of the mares uterus occurs very rapidly after foaling in comparison to the cows. By the beginning of foal heat, it should be no more than two to three times its normal size. Other causes of a uniformly enlarged uterus are pyometra and pneumo uterus.
Discrete Uterine Enlargements
Discrete uterine enlargements must be differentiated from early pregnancy by identifying the embryo as a discrete bulge in the uterine horn.
Other enlargements include:
- endometrial cysts (result from blocked and dilated endometrial glands).
- lymphatic lacunae (which result from blocked lymph channels).
- abscesses in the uterine wall and corneal dilatation (following atrophy of the uterine mucosa in older mares).
Parauterine Abnormalities
- Parauterine abnormalities include haematoma in the broad ligament of the uterus that are usually associated with parturition.
- A fresh hematoma should not be disturbed, and the mare should be treated with systemic antibiotics to prevent abscessation.
- A chronic hematoma rarely causes a fertility problem and usually regresses over time.
Abnormalities Involving Ovaries
Ovarian abnormalities identified on physical examination can be divided into small ovaries and large ovaries.
Small Ovaries
These may be either normal or abnormal. Prepubertal or juvenile ovaries are small; therefore, the age and previous cyclic history of the mare is important.
In anestrus the ovaries are inactive and one half the size they will attain during the breeding season. In some small, docile, chronically anestrus mares a chromosomal anomaly called XO Gonadal dysgenesis may be the cause of small ovaries. An endometrial biopsy from these mares often demonstrates glandular insufficiency.
‘True’ nymphomaniac mares also contain smal ovaries. These mares act as if they are in persistent estrus, yet often they will not allow mounting; some of these mares will demonstrate male like behavior. Other than small, firm ovaries, no other abnormalities of the genital tract are noted in the nymphomaniac mare.
Enlarged Ovaries
- May be a seasonal phenomenone. During the transitional periods, follicles may grow to abnormally large sizes and persist for various lengths of time before ovulating or regressing
- They usually do not suppress activity in the other ovary and resolve themselves and cause no permanent problem.
- In the early transition period they can be treated with 1000 to 5000 IU of Human Chorionic Gonadotrophin but results are variable. These persistent follicles are often diagnosed as cystic ovaries by practitioners unaccustomed to palpating the mare‘s ovaries.
- Cystic ovaries, such as those that occur in cows, do not occur in mares. The biggest problem in dealing with persistent follicles in mares is differentiating them from certain types of ovarian tumors.
Ovarian tumors
- In the mare ovarian tumors are usually classified according to the main type of cell making up the tumor. Most of these tumors are unilateral and rarely malignant
- The cystadenoma must be differentiated from persistent follicles. These usually enlarge over a period of time unlike the persistent follicle that remains the same or regresses. They probably arise from the surface epithelium of the ovary or the rete ovarii and have one or several large fluid-filled cavities within them. Diagnosis is by ultrasound treatment is only ovariectomy.
Ranulose (theca cell tumors)
- Most common ovarian tumor in the mare.
- Grow to very large sizes and are usually unilateral and benign.
- Produce a variety of hormones and usually suppress activity of the opposite ovary.
- In addition to secreting inhibin, these tumors frequently secrete testosterone causing the mare to exhibit stallion-like behavior.
- Hormonal analysis and endometrial biopsy may also be helpful in diagnosing this tumor.
- Clinical signs vary from anestrus to nymphomania and even to virility depending on the predominant hormone produced by these tumors.
- Treatment is removal of the affected ovary, and the prognosis for fertility is fair to good, depending on the length of time that the tumor has existed and the degree of suppression of the opposite ovary. Resumption of cycle occurs 1 to 4 month after the tumor is removed.
- Much less common ovarian tumors are teratoma and the dysgerminoma.
Teratoma
The teratoma is a multiple tissue type tumor that usually has epithelial structures including cartilage, bone, hair and glandular epithelium.
Are usually benign and produce no hormones, so the contralateral ovary usually remains functional, and the mare may continue to cycle. As in the other ovarian tumors, ovariectomy is indicated.
Dysgerminoma
- Unlike the previously discussed ovarian tumors, the dysgerminoma can be malignant.
- It arises from the germinal epithelium of the ovary and can become very large. The tumors may be solid or contain fluid-filled multiple cysts. Ovariectomy is the treatment of choice.
Non-Neoplastic Ovarian Enlargements
- Other causes of ovarian enlargement such as non-neoplastic ovarian abscesses and hematoma are common and are difficult to differentiate.
- The mare‘s temperature and white blood cell count may help identify the ovarian abscess, yet these abscesses are often encapsulated within the ovary and do not produce a systemic reaction after they become chronic.
- Ovarian hematomas often feel similar to ovarian abscesses. In both cases the opposite ovary usually remains functional and the mare continues to cycle. Ovarian hematomas usually regress over a period of time and cause no fertility problems.
- Hormone stimulation tests may differentiate these from ovarian tumors. An ultrasound examination may be of some help in differentiating them.
- The last cause of ovarian enlargement that should not be overlooked is the unusually large, normal cyclic follicle. Most cyclic follicles range in size from 2.5 to 6 cm in diameter prior to ovulation.
- Occasionally, one or several large follicles grow to 10 cm or more before ovulation. In this and all cases of ovarian enlargement, several examinations over a 15 to 30 day period are a valuable means of differentiating these ovarian abnormalities.
Abnormalities Involving Oviduct
The incidence and abnormalities of salphingitis and hydrosalpinx seems to be very low when compared with cattle.
Fimbrial cysts are not a rare finding in the mare. These are usually small and inconsequential. Occasionally, they may grow large enough to interfere with the collection of the ovum by the fimbria.
Cervical Abnormalities
When evaluating the cervix, the normal pinkness of estrus must be differentiated from the redness of inflammation.
Cervicitis may be caused by contagious equine metritis, endometritis or vaginitis or may be secondary to pneumo vagina or recto vaginal fistula.
The most common non-infectious abnormalities noted are cervical adhesions and scars secondary to foaling or breeding problems.
These abnormalities may prevent the cervix from opening and/or closing properly dilate thereby:
- preventing the stallion from ejaculating into the uterus.
- making delivery of a foal difficult.
- predisposing the mare to endometritis which may prevent her from carrying a foal to term.
Other abnormalities of the cervix include leiomyoma of the cervix and squamous cell carcinomas.
Vaginal Abnormalities
Scars, adhesions and lacerations are some of the more common vaginal abnormalities that may lead to difficulies in foaling and breeding.
Lacerations subsequent to breeding often occur in the fornix of the vagina; are usually retroperitoneal and heal well.
Recto vaginal fistula, which is a foaling accident, occurs as a result of the foal sticking a foot through the dorsal wall of the vagina and through the ventral floor of the rectum. If the foot is not withdrawn into the vagina, the entire perineal body between the rectum and vagina may be torn, producing a third degree perineal laceration.
Other vaginal problems encountered are:
- pneumovagina secondary to cervicitis and endometritis. Caslick‘s operation is performed routinely on many farms and may be one of the best management aids to overcome the problem of the barren mare.
- Vaginal abscesses occasionally occur subsequent to a vaginal laceration. They should be drained into the vagina, with care taken to avoid the large perivaginal blood vessels. Systemic and local antibiotics should be used to speed healing.
- Persistent hymen can be identified by vaginoscopy. Correction involves manually or surgically dilating the hymen. Prepartum vaginal prolapse is rare in the mare.
- Occasionally, a persistent hymen, perivaginal abscess or hematoma may be mistaken for a vaginal prolapse.
Vulvar Abnormalities
Dorsocranial slope associated with pneumovagina is the most common vulvar abnormality encountered. At least 70 per cent of the vulvar cleft should be below the brim of the pelvis.
Abnormal labial apposition can result in the same problems as abnormal slope and should be corrected by Caslick‘s operation. Occasionally, a mare will be encountered that has suffered a severe vulvar laceration because an episiotomy was not performed on a mare that has had Caslick‘s operation.
Third degree perineal lacerations involve the vulva. Reconstructive surgery should be attempted. Clitoral hypertrophy is occasionally seen in fillies. This is usually a manifestation of pseudohermaphroditism.
Neoplasia of the vulva include fibromas or fibropapillomas, malignant melanomas and squamous cell carcinomas.
Ultrasonography
Can be used to identify the amniotic vesicle as early as day 15 of gestation and is valuable in predicting the presence of twins early enough in gestation to correct the problem without danger to the mare.
Also helpful in producing an image of various vaginal, uterine and ovarian masses to determine if they are solid or fluid filled.
Hormonal and Chromosomal Analysis
- Analysis for progesterone, estrogen and/or testosterone may be of value in differentiating the several causes of enlarged ovaries.
- Detection of pregnancy with pregnant mare serum gonadotrophin requires a blood test.
- Chromosomal analysis may be of value in ruling out specific cases of persistent anestrus in mares.