TABLE OF CONTENTS
Postural Abnormalities Causing Dystocia: Common Forms and Clinical Insights
Postural abnormalities are a common cause of dystocia, particularly in large animals such as cattle, buffaloes, and mares.
Common forms of dystocia due to postural abnormalities include:
- Lateral Deviations of Head and Neck
- Downward Deviation of Head
- Deviation of the Forelimb
- Carpal Flexion Posture
- Shoulder Flexion Posture
- Hock Flexion
- Hip Flexion (Breech Presentation)
1. Lateral Deviations of Head and Neck
Deviations of head and neck are common types of abnormal posture in anterior presentation causing dystocia in all species.
In swine because the neck is so short this type of dystocia is very rare.
Diagnosis
- In cow, this condition is easily diagnosed by finding the two fore limbs in the birth canal but not the head.
- By passing the hand and arm alongside the fetal body as far as possible and then carrying it around the body, the head and neck are found and the direction of the deviation determined.
- In mare this may be more difficult because the head is usually out of reach of the hand.
- By locating the withers, mane and trachea of fetus these may be followed to the left or right.
Correction
- If the bovine fetus is alive, the deviation may be corrected with least amount of difficulty.
- This is performed under epidural anaesthesia with the animal standing.
- If the animal is down it should be placed in lateral recumbency with rear parts higher, with the fetal head in the upper flank of the dam above the fetal body.
- In more protracted cases of head displacement with greater loss of fetal fluid, fluid substitute renders the calf more buoyant.
- The fetus is repelled by pushing forwards at the base of its neck.
- The hand is then quickly transferred to the muzzle of the calf, which is firmly grasped and brought in line with the birth canal.
- The incisor teeth should be guarded to prevent laceration of the uterus.
- In a more inaccessible case the mandibular snare is applied. Care should be taken to apply the snare below the tongue and traction is applied to bring the head in line with the birth canal.
- Alternatively a head snare is applied and the fore limbs are now affixed and traction synchronously applied with the cow‟s expulsive effort, to deliver.
- If mutation fails because the fetus is emphysematous or because the uterine wall is contracted tightly around the fetus fetotomy and amputation of the head and neck is indicated.
2. Downward Deviation of Head
Downward deviation of the head between the fore limbs is occasionally seen in all species except swine.
Diagnosis
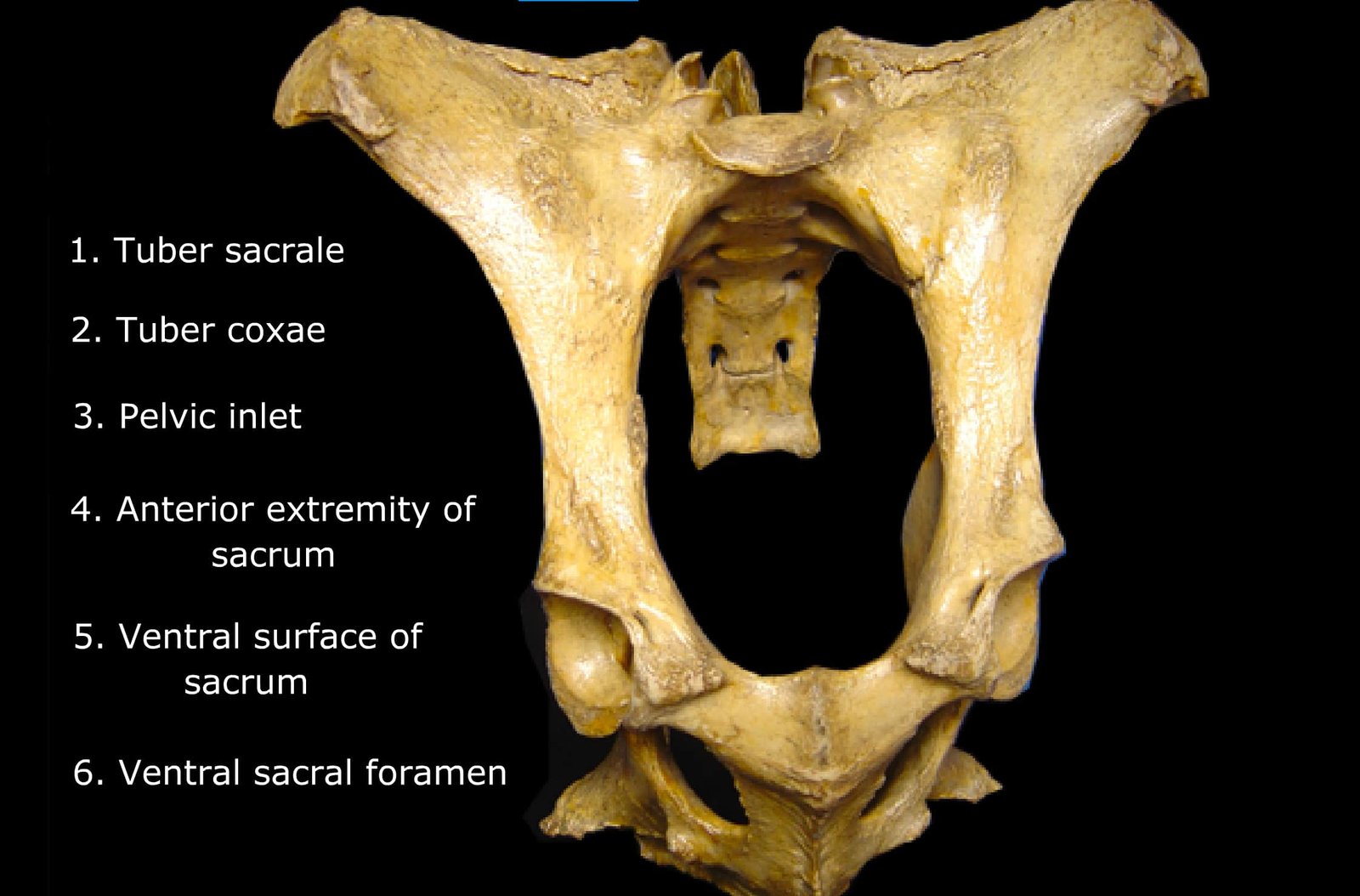
- In mild case, only the nose of the fetus is caught on the brim of the pelvis with the forehead entering the pelvic in let-vertex presentation.
- In severe flexing of head and necks, the ears and the poll of the head are presented-poll posture.
- In more severe cases the neck extends between the fore limbs and the head is against the fetal sternum or abdomen-Nape posture.
- In this type of nape posture the fore limbs do not came together and that in the mare the mane of the fetus may be felt between the legs.
Correction
- Repelling the fetus and grasping the muzzle of the fetus and raising it into the pelvic cavity usually correct vertex posture and poll presentation.
- Neglected cases may require epidural anesthesia and fetal fluid supplement.
- During the correction of nape after the fetus is repelled, a forelimb may be flexed alongside the body.
- This gives room for the head to be rotated laterally and then brought upward and forward over the pelvic brim.
- The leg is then extended and the fetus removed by traction.
- In very difficult case it may be advantageous to replace both forelimbs into the uterus.
- Casting the cow and placing her in dorsal recumbency greatly facilitate extension of fetal head.
- When manipulative delivery fails, fetotomy may be done.
3. Deviation of the Forelimb
- These are relatively common cause of dystocia in uniparous animals.
- They are rarely seen in multiparous animals because their forelimbs are short and flexible.
4. Carpal Flexion Posture
- One or both limbs may be affected.
- In unilateral cases the flexed carpus is engaged at the pelvic inlet and the other foot may be visible at the vulva.

Correction requires retropulsion of the fetal head and the retained foot is then grasped and as the carpus is pushed upwards the foot is carried outwards, forwards and extended alongside the other limb.
More difficult case requires a snare attached to the retained fetlock to help extend the limb.
5. Shoulder Flexion Posture
- This type of dystocia may be unilateral or bilateral.
- The diagnosis of bilateral retention is usually obvious by observing that the head is party or completely born, but there is no sign of feet.

Correction
- Retropulsion is necessary and if the head is much swollen, the calf being dead the head should be amputated outside the vulva.
- Following repulsion the calf forearm is grasped and the defect is easily converted into carpal flexion and the relived.
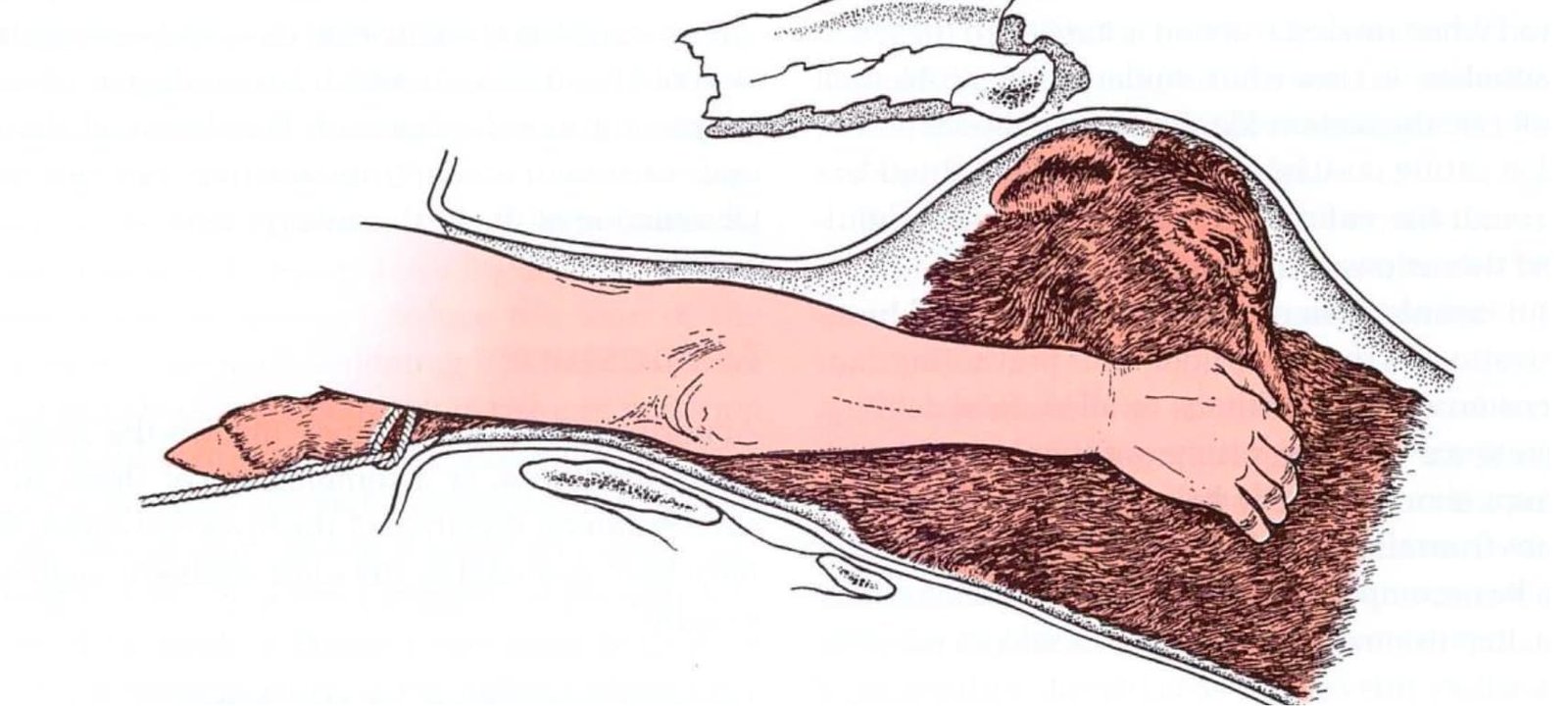
6. Hock Flexion
Hock flexion condition is usually bilateral. They are caused by failure of the hind limbs to extend into the pelvic cavity or by the foot or fetlock catching on the birth canal or pelvic brim; causing the hind limbs to become flexed.
Diagnosis
Hock flexion may be diagnosed by palpation of the perineal region and tail of the fetus on vaginal examination.
Correction
- The fetus is first repelled by pressing forward in its perineum and the hand then grasps the fetal foot.
- As the foot is drawn back through, the hock is firmly flexed and retropulsion maintained as far as possible.
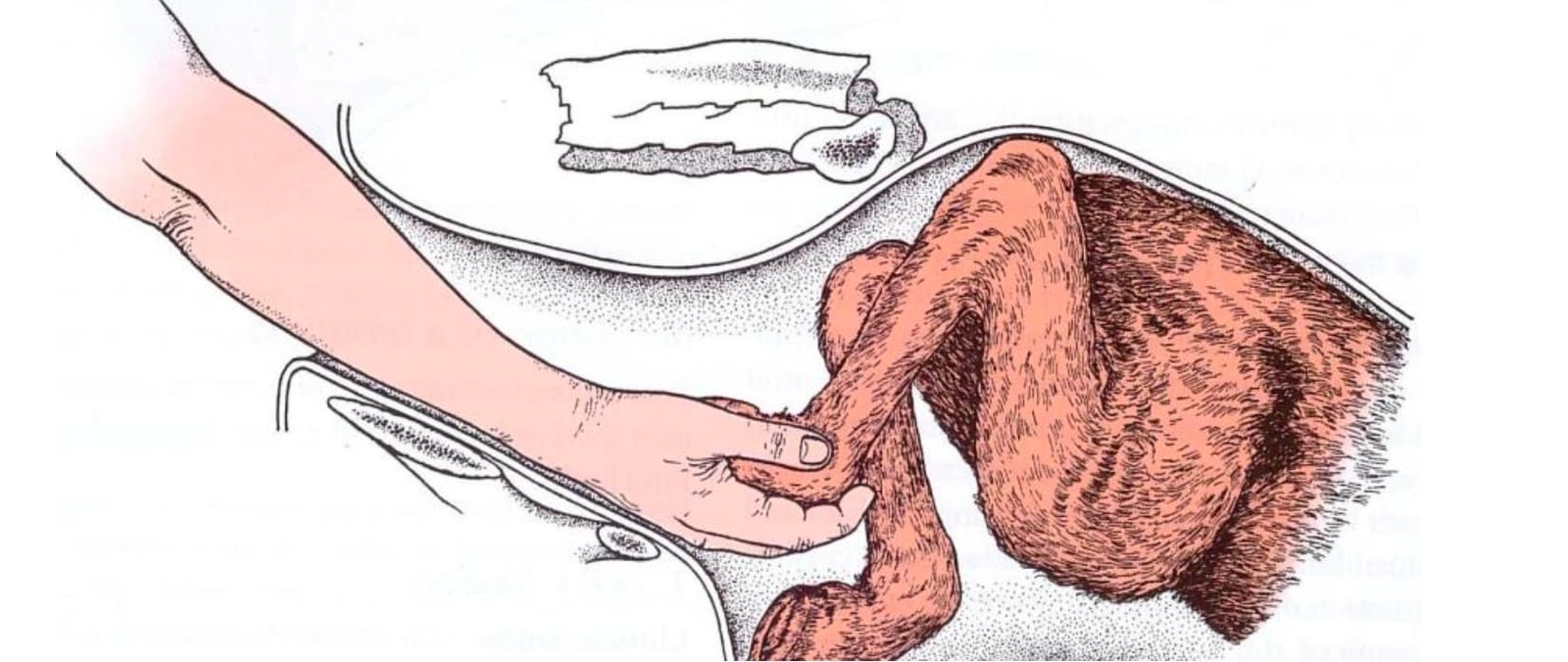
- Eventually with the digit in the cupped hand the foot is lifted over the pelvic brim and the limb extended in the vagina.
- An alternate method is to supplement manual extension by traction on a snare fixed to the retained foot on the pastern and the snare is placed between the digits so that when traction is applied to it the fetlock and pasterns joints are flexed.
- Now the flexed hock is grasped and repelled forward, while the foot is drawn caudally and extended through the birth canal.
- In occasional case where it is impossible to extend the hock simple foetotomy may be performed. Achilles tendon may be severed so as to make maximum possible flexion or the limb may be amputated below the point of hock by means of wire saw.
7. Hip Flexion (Breech Presentation)
- The rear limbs are completely extended beneath the foetus. Usually both hind legs are retained in the uterus than unilateral retention.
- On vaginal examination the buttocks and tail are in the pelvic cavity and occasionally the tip of the tail is hanging from the vulva. In many cases no part of the limb can be reached until the buttocks are repelled cranially out of the pelvic inlet.
Correction
- The aim of the treatment is to convert the condition into one of the hock flexion posture.
- The manipulative procedure is to repel the calf perineum forwards and upwards with a view to bring the retained limbs within reach, by grasping the cranial aspect of the tibia with the hand or pass a snare around the tibia and pull the fetal leg back into hock flexion posture. Now the hock flexion can be relieved as described previously.