TABLE OF CONTENTS
Mastitis in Dogs
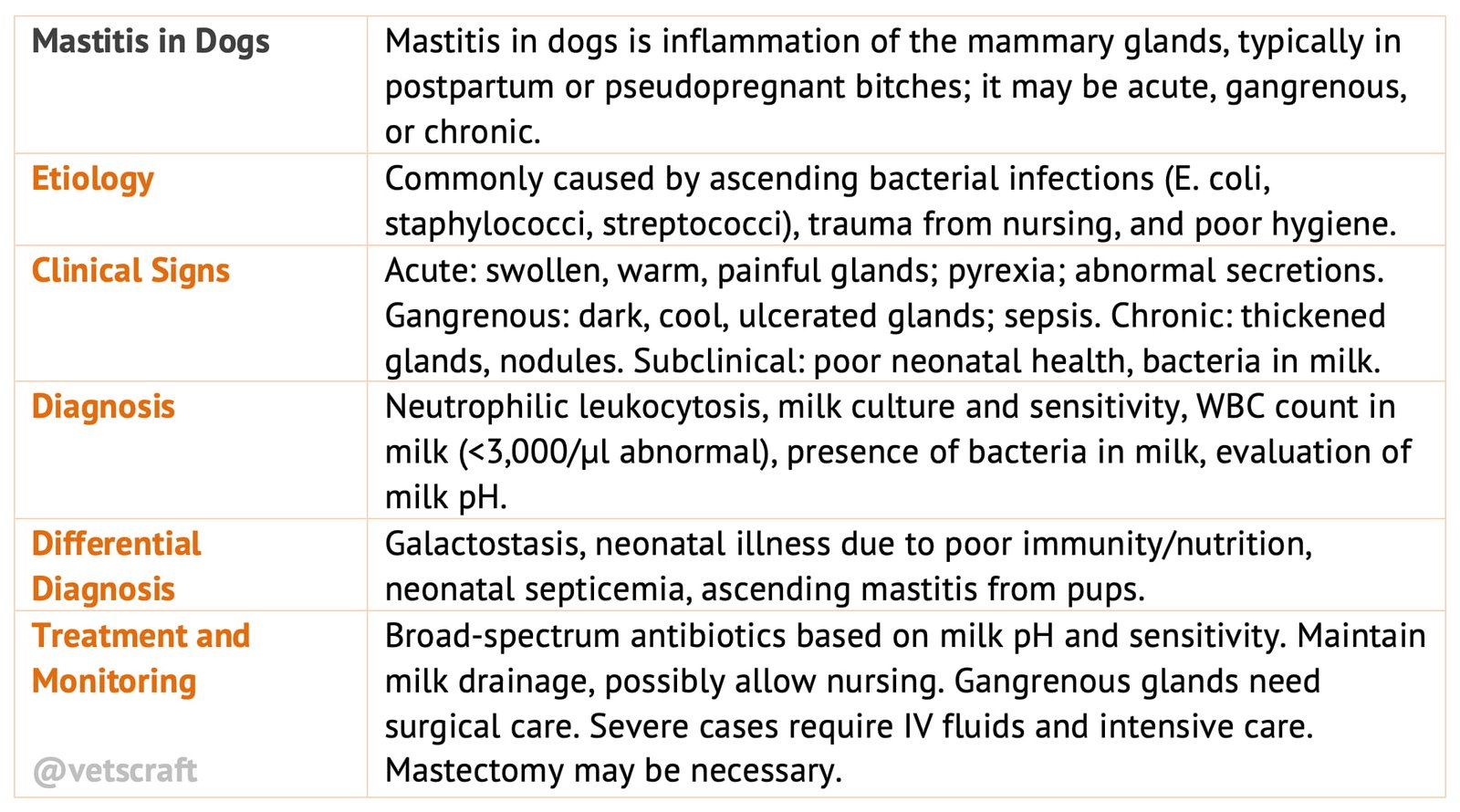
Mastitis in dogs is the inflammation of the mammary glands. It is a condition primarily restricted to the postpartum or pseudopregnant bitch.
Mastitis in a female dog may occur in the acute, gangrenous or chronic forms. The incidence or significance of sub clinical mastitis is not known.
Etiology
- Ascending bacterial infection, via the teat orifices and hematogenous spread are the most likely causes
- Coliforms (especially Escherichia coli), staphylococci and streptococci are most commonly isolated from infected milk.
- Trauma from nursing pups as well as poor hygiene may contribute to mastitis.
Clinical Signs
Acute Mastitis
- One or more warm, painful, reddened and swollen glands are present; the caudal glands are more often affected.
- Pyrexia may be present.
- Dams may be presented owing to neonate morbidity or mortality.
- There may be secretions from affected gland(s). not all portions of the gland may be inflamed; thus not all test orifices may yield an abnormal discharge.
- Brownish, hemorrhagic, or purulent secretions may be expressed.
Abscesses or Gangrenous Changes
- Affected glands may be dark, cool and / or ulcerated.
- Signs of systemic sepsis may be present.
Chronic and Sub Clinical Mastitis
- Chronic bacterial mastitis may be an incidental finding in older, non lactating queens.
- Inflammatory changes are usually minimal. Affected glands may appear thickened and nodules may be palpable. Grossly these changes are indistinguishable from mammary neoplasia.
- Subclinical bacterial mastitis should be suspected in asymptomatic lactating dam whose young are presented for poor weight gain or other unexplained septic illness.
- Bacteria, leukocytes and macrophages are found in the milk.
- It is unclear if this form of mastitis is a cause or effect of bacterial disease in the nursing neonate.
Diagnosis
Hemograms from dams with acute bacterial mastits generally show a neutrophilic lukocytosis.
Fluid analysis and culture of abnormal gland secretions are useful. Estimated white blood cells (WBC) counts <3,000/µl are considered abnormal. Degenerate neutrophils are the predominant cell type noted.
Elevated WBC counts in milk are occasionally noted in normal dams as well as in those with galactostasis. Phagocytized bacteria within degenerative polymorphs and macrophages are commonly found in mastitic milk.
Bacterial culture and sensitivity and evaluation of the pH of infected milk aid in antimicrobial selection.
Differential Diagnosis
Mastitis in a lactating dam must be considered in the differential diagnosis associated with illness or death in nursing neonates.
- Bitches with acute mastitis may provide inadequate passive immunity, nutrition and hydration to their young.
- Ingestion of infected milk is a suggested, although unproved, cause of meonatal septicemia.
Theoretically, pups with bacterial diseases may cause ascending mastitis in the dam via suckling.
Many of the clinical signs of galactostasis are similar to those of bacterial mastitis.
Treatment and Monitoring
Give broad-spectrum antibiotics, based on culture results.
Evaluation of milk pH may be important in antibiotic selection:
- If milk is more acidic than normal plasma pH (dogs <7.3; cats >7.2), antibiotics that are weak bases are indicated.
- Trimethoprim-sulfadiazine combination 15-30 mg/kg PO BID x 21 days.
- Erythromycin 10 mg/kg PO TID x 21 days.
- Lincomycin 15 mg/kg PO TID x 21 days.
- If milk is more alkaline than normal plasma (pH >7.4), antibiotics that are weak acids are indicated.
- Ampicillin 20 mg/kg PO TID x 21 days.
- Cephalexin 30 mg/kg PO TID x 21 days.
- Tetracycline HCI 10 mg/kg PO TID or doxcycline 5-15 mg/kg PO BID and chloramphenicol 50 mg/kg PO (dogs TID, cats BID) x 21 days appear in the milk in reasonable concentrations independent of pH.
- Tetracycline may cause yellow staining of tooth enamel in nursing pups and kittens.
Aminoglycosides are not recommended owing to poor penetration of the blood mammary gland barrier.
These consideration may be less significant in the acutely inflamed mammary gland because of break down of the milk plasma barriers.
With chronic or relapsing infections culture and sensitivity and milk pH evaluations are critical for effective therapy.
Keeping the affected gland(s) empty of abnormal secretions is important. Milking may be performed manually by the owner.
It is controversial whether the young should be allowed to nurse from the mastitic gland(s). Most authors suggest continuation of nursing in the absence of abscessation or gangrene. Ingestion of either infected secretions or milk containing antibiotics is rarely a problem to the young. Affected milk does have a poor nutritional content, however.
Gangrenous or abscessed mammary glands require further therapy. They may be a sequel to progressive, acute mastitis.
Anaerobic organisms may play a role. Treat with surgical drainage and warm antiseptic compresses.
Remove glandular secretions BID and prevent offspring from nursing.
Infuse affected gland(s) with antibiotics or antiseptic solution (0.5-1.0% povidone iodine) BID for 2-5 days. Find affected test orifice. A lacrimal duct cannal or small gauge polyethylene catheter may be used.
Chronic, persistently infected glands may ultimately require mastectomy.
Signs of septicemia demand aggressive support with intravenous fluids, appropriate antibiotic therapy, and intensive nursing care.
If offspring are prevented from nursing, owners are offered advice regarding hand rearing techniques.