TABLE OF CONTENTS
Congestive Heart Failure (CHF)
Congestive heart failure (CHF) is a complex clinical condition characterized by inefficient myocardial contractions, resulting in compromised blood supply to the body and development of congestion.
Etiology
- Valvular disease like Endocarditis, Congenital valvular defects or Rupture of valve or valve chordae.
- Myocardial diseases like Myocarditis, Myocardial degeneration, Congenital or hereditary cardiomyopathy or Toxins affecting cardiac conduction.
- Congenital anatomical defects producing shunts.
- Hypertension
- Pressure load
- Volume load
- Pumping defects (systolic failure)
- Filling defects (diastolic failure)
Pathogenesis
Congestive heart failure (CHF) may be right sided or left sided. According to this pathogenesis also varies.
Clinical Findings
- Respiratory distress on light exertion
- Tachycardia
- Loss of body weight
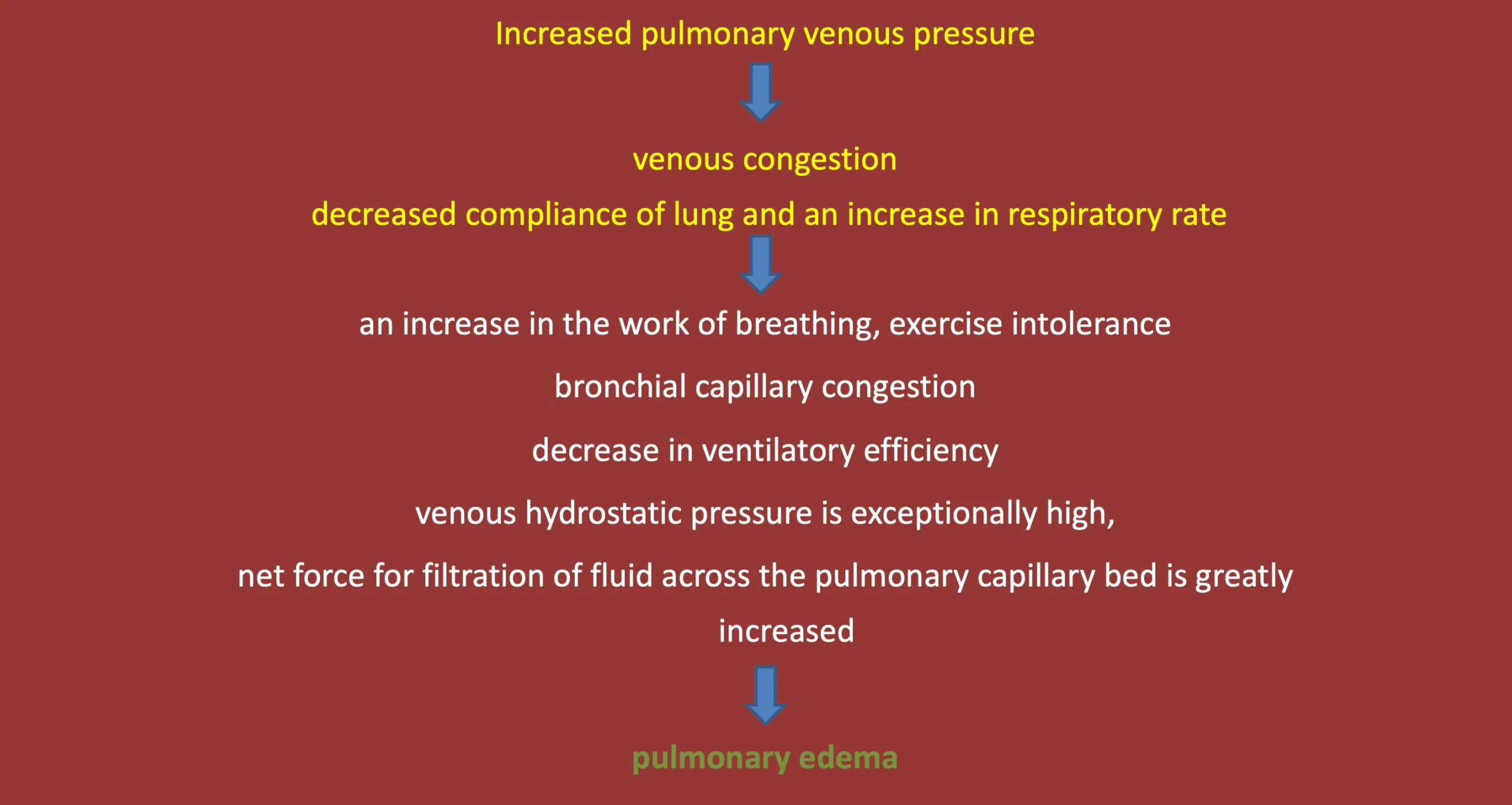
Clinical findings in left-sided CHF:
- Tachycardia
- Increase in rate & depth of respiration at rest
- Cough
- Presence of crackles (discontinuous sounds) at the base of the lungs
- Increased dullness on percussion of the ventral borders of the lungs
- Severe dyspnea and cyanosis
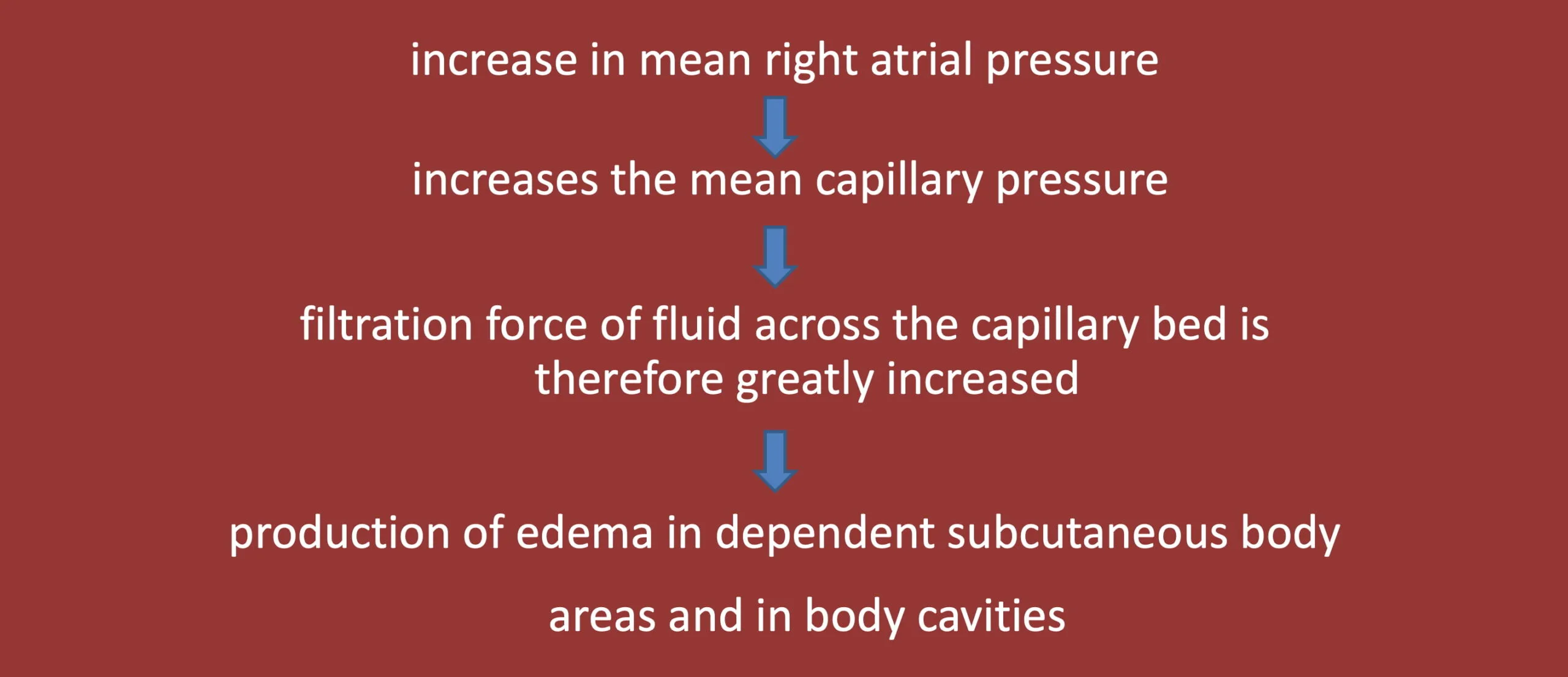
Clinical findings in right-sided CHF:
- Engorgement of superficial veins
- Subcutaneous edema
- Ascites
- Hepatomegaly
- Epistaxis and exercise intolerance esp. horse, dogs
Diagnosis
- Examination of fluid effusion
- Edematous transudate except in pericardial tamponade (serosanguinous) or pericarditis (effusion). it may be septic or non-septic.
- Protein in urine
- Cardiac troponin I provides an excellent cardiac biomarker in large animals
Necropsy Findings
- Left-sided CHF: Pulmonary congestion and edema
- Right-sided CHF: Anasarca, ascites, hydrothorax and hydropericardium Enlargement or engorgement of liver, with ‘nutmeg’ appearance.
Prognosis
- Poor to Grave
- Animal survive with a permanently reduced cardiac reserve
Treatment
- Pericarditis or pericardial tamponade to removing the pericardial fluid and preventing its return.
- Reducing effects of increased preload by administering diuretic agents (like frusemide) and restricting sodium intake.
- Advise rest
- Oxygen supplementation
- Reduction of pulmonary venous pressure with IV frusemide 2-8 mg/kg in severe pulmonary edema then reduced to 2-4 mg/kg every 8-12 hours
- Vasodilator like sodium nitroprusside
- Sympathomimetics (Dobutamine 5-15 µg/kg/min in 5% dextrose and Dopamine 1-2 µg/kg/min)
- ACE inhibitors like Enalapril (0.5 mg/kg PO BID), Benazepril (0.25-0.5 mg/kg/day PO)
- Positive inotropes like Digoxin(0.003-0.005 mg/kg initially)
- Pimobendan (0.2-0.3mg/kg PO BID

