TABLE OF CONTENTS
Retained Fetal Membranes (RFM) in Cows: Causes, Symptoms, Treatment & Prevention
Retained fetal membranes (RFM) or retained placenta in cows is defined as the failure of the villi of the fetal cotyledon to detach from the maternal crypts of the caruncles and retained longer than physiological time limits.
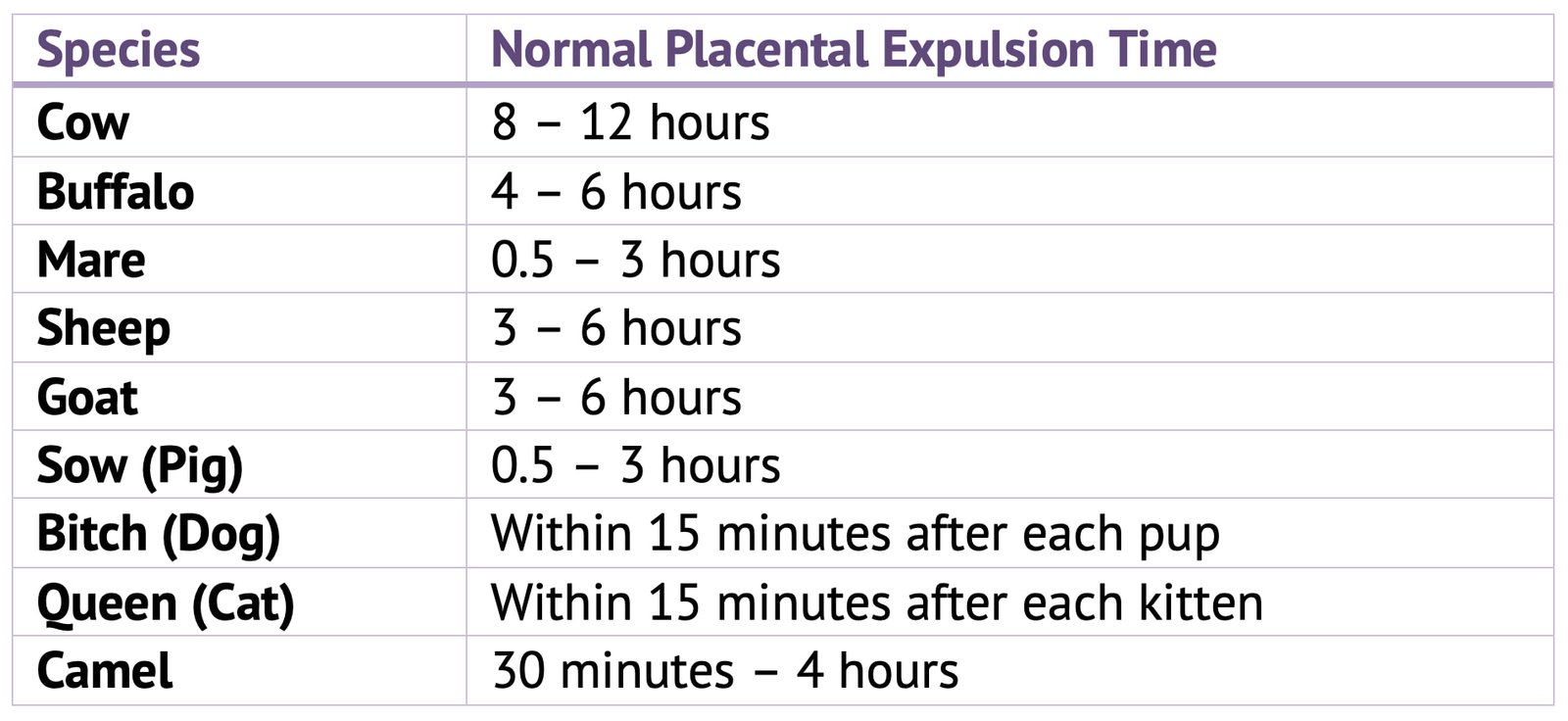
Normal placental expulsion time in various animals:
Incidence
Retained fetal membranes (RFM) is most common in dairy cows but can occur in other species like, mare, sow, sheep, goat and pigs.
Mechanism of Shedding of Foetal and Maternal Membranes
Normally shedding of placenta takes place in two phases:
- Separation of placenta from endometrium
- Expulsion of placenta by uterine contraction
After the fetus is expelled and the umbilical card ruptures, no blood is pumped into the foetal villi and they shrink in size. In dam the larger amount of blood formerly going to the uterus is markedly reduced and the maternal crypts dilate. Hence, the shrinking villi detached from dilated maternal crypts. This detached foetal membranes expelled out by uterine contractions.
Degeneration and necrosis of the fetal villi and the epithelium of the maternal crypts due to autolysis by enzymes soon after calving, also aided in the detachment.
Etiology
General Causes
Infectious causes: Infections of uterus during gestation may be a cause for retained placenta. Infectious agents such as brucellosis, vibriosis, leptospirosis, IBR-IPV and various moulds causing severe retention of the fetal membranes by inflammatory reactions of the cotyledon and caruncles.
Nutritional cases: Selenium and Vitamin A is necessary for maintaining the health and resistance of the epithelium of the uterus and placenta. In cattle the low level of carotene lead to vitamin ‘A’ deficiency, lead to the development of infection or abortion and premature birth causes retention of placenta. Lack of minerals such Iodine causes retained placenta.
Hormonal causes: The progressive deficiency or an excess cortisol in late gestation may cause the retention of fetal membranes by predisposing to early parturition.
Diseases: Diseases like dropsy of the fetal membranes, uterine torsion, fetal piantism, dystocia, debility, old age and other pathological conditions, causing uterine inertia or atony results in a high incidence of retention of foetal membranes.
Miscellaneous Causes:
- Hereditary: Less common in beef breeds than in dairy head.
- Sex of the calf: Male calf more prone for retained placenta.
- Season: More common during April to May calvings.
- Confinement: Close confinement and lack of exercise highly prone for retained placenta.
Precise Causes

Recent Concepts for Causing RFM
- Weight loss/gain during the dry period has been hypothesized as a risk factor for RFM.
- Changes in energy balance are felt to influence the degree of hypertrophication and interdigitation of the microvilli of cotyledons with the crypts of the caruncles.
- Actual separation of the placenta starts well before the actual calving event.
Clinical Signs
The symptoms of retained placenta are usually obvious. A portion of the fetal membrane hangs from the vulva 12 hours or more even after the expulsion of the foetus.
Occasionally the foetal membranes do not hang from the vulva but are entirely within the vagina or uterus.
Some animals show symptoms of anorexia, depression, elevation of body temperature and increase in pulse rates.
A fetid purified odour develops since the placenta begins to macerate after 24 hours of foetal expulsion.
Duration of retention depends on:
- Extent of the areas of attachment of the fetal membranes
- Rate of uterine involution
- Amount of uterine exudates, and
- Proportion of the afterbirth which had already passed through the cervix when retention began.
The toxic products of putrefaction accumulate within the uterus causing a fetid odour which pervade the atmosphere and, more importantly, taints the milk, and makes it unacceptable for human consumption.
Delayed involution of the uterus and a variable degree of metritis commonly accompany retention.
In cows with RFM which have calved spontaneously after a normal length of gestation there are subtle changes in health. Whereas, if retention occurs following extensive assisted delivery in dystocia, a severe metritis and toxaemia can supervene within 2 or 3 days which, if untreated, can be fatal.
If RFM is accompanied by metritis, the symptoms depend upon the severity of the uterine disease.
Prognosis
- Fair to good if properly treated.
- There is slight to moderate delay in the involution of the uterus and subsequent conception.
Treatment
- Manual removal
- Without manual removal-shed on its own accord. Allowing the placenta to be voided on its own accord is not practicable in tropical countries.
Manual Removal
Manual removal can be attempted in 24-48 hours after parturition. Manual removal after 48 hours is not advisable because cervix was closed and it is difficult or impossible to insert the hand into the uterus if no foetal membranes are within the cervix.
- The operator should wear a surgical rubber glove or a disposable glove and long sleeve on other arm to protect himself from the infection of the arm or hand.
- The perineal region of the cow should be carefully cleaned and washed with soap, water and mixed antiseptic and kept clean during operation.
- To prevent straining epidural anaesthesia may be helpful.
- The free part of the fetal membranes should be drawn through the cervix thereby reducing the amount of membrane in the uterus and aiding manual attempt to detach the fetal placenta.
- The hand is inserted between the endometrium and the chorion in the intercotyledonery space and the individual fetal cotyledon and its caruncle are grasped gently and the two structures are gently separated by a rolling, pushing and squeezing motion. This may be aided by traction with the other hand on the adjacent portions of the fetal membranes. The cotyledons in the cervical area of the uterus are removed from the carunules as the cotyledons in the middle portion of the horn and the non-gravid horn are removed.
- Manual attempt to detach the fetal placenta from the maternal caruncles should be done carefully. Some injuries to the endometrium may result and the risk of toxaemia and septicaemia is thereby increase.
- Placental removal must be gently, quick (5-20 mts) with maximum possible antiseptic precautions and with a few withdrawals and reintroduction of the arm as possible.
- If the operation cannot be performed in a gentle manner, the fetal membranes should be left as such even though the cervix may contract. The membrane should be allowed to fall away naturally after the maternal caruncle and foetal cotyledons have separated from the uterine wall by autolysis. Even if the membranes or a portion of them macerated and are absorbed in the uterus, this is better than severely traumatising the uterus and cervix.
- Douching the uterus is contraindicated before complete removal of the placenta.
- Administration of parenteral or local antibiotic.
- Hormones:
- Oxytocin 30-40 IU s/c or i/v in drips and calcium borogluconate.
- Estrogen 10-20 mg.
- PGF2α
- Intrauterine antiseptic have been used locally to control the bacterial flora in the uterus.
- Ecbolic drugs.
Contraindications for Manual Removal
- Elevated body temperature above 103° F
- In severe necrotic vaginitis and vulvitis
- Septic metritis
- Acute mastitis
- Traumatic gastritis
Current Recommendations
- Cows should not be examined until 96 hours after calving and that removal should be gentle.
- It should be limited to the withdrawal of the membranes from the genital tract after they have become spontaneously detached from the caruncles.
- In many animals, spontaneous detachment may have occurred within 96 hour, it is acceptable to leave the placental membranes for 10 or even 15 days before removal, if this length of time was needed for their detachment.
Antibiotics
- One antibiotic of choice is tetracycline @ 2-6 gm intrauterine.
- Treatment should begin 12 hours postpartum and continue daily until total expulsion of the membranes.
- Systemic penicillin (amoxicillin) can be given for possible septicemia.
Ecbolic Agents
- To physically cause the caruncle and cotyledon to separate, Oxytocin and Prostaglandin F2α injections are used within 72 hours of parturition.
Oxytocin
- Oxytocin injections (20-40 IU) are continued for 3 days after calving to contract an estrogen primed uterus.
- It should be given as IM injections in small doses and often.
High doses exaggerate uterine contractions, may force premature closure of the caruncles, and favours retention.
Note that oxytocin therapy will not be effective if tried 3-4 days after parturition. So ergot preparation can be given after 3-4 days parturition.
Prostaglandin F2α (PGF2α)
- After 3 days, 25 mg of PGF2α injections must be administered IM.
- It can be administered once or twice a day. PGF2α are used because there is no withholding time for milk.
- Multiple injections stimulate myometrial contractions and luteolysis for a return to oestrus.
Administration of Collagenase
An injection of collagenase into the umbilical artery duplicates the cow’s response to release the cotyledons from the caruncles or 200,000 units/litre with 500 mg of calcium chloride is infused into one or both the uterine horns between 24-36 hours postpartum.
Preventive Approach
- Supplementation of anionic salts to the diet. RFM is thought to be influenced by electrolyte concentrations.
- Uncomplicated cases of RFM require no treatment.