TABLE OF CONTENTS
Hydrallantois
Hydrallantois is characterized by sudden and excessive fluid accumulation in the allantoic cavity. This condition is seen sporadically in dairy and beef cattle.
Etiology and Pathogenesis
Hydrallantois is usually associated with a diseased uterus in which most of the caruncles in one horn are not functional and the rest of the placentomes are greatly enlarged and possibly diseased.
- Adventitious placentae are commonly observed.
- Commonly seen in cattle carrying twin foetuses.
- Hydrallantois is caused by structural or functional changes in the allantois-chorion including its blood vessels.
- It results in transudation and collection of fluid, differing from normal allantoic fluid but resembling plasma.
- Fetal kidneys seldom play a role in causing this disease. The presence of cystic kidneys, hydronephrosis or dysfunction of the fetal renal tubules resulting in polyuria might be concerned with the pathogenesis of hydrallantois.
- Vitamin ‘A’ deficiency resulting in a lowered resistance of the endometrium leading to hydrallantois.
- Hydrallantois usually affects older age cows although it rarely seen in heifers in which congenital lack of caruncles was present.
- In older cows, this lack of caruncles characteristic of hydrallantois may be due to prior uterine infection or even tuberculous metritis.
Clinical Signs
In mid cases, where the amount of fluid is moderate (40 – 80 litres), the condition may not be diagnosed until parturition. At this time, an excessive amount of clear, watery, amber color fluid with the characteristics of transudate is expelled. The fetal membranes may be tough and rupture with difficulty.
The uterus is greatly enlarged and atonic and fetus may exhibit some edema and ascites. Dystocia may occur at the time of abortion / parturition due to inertia. The fetus is usually dead at birth or dies shortly thereafter.
In severe cases, symptoms of hydrops of allantois may occur as early as fifth month of pregnancy.
Hydrallantois rapidly develops within 5-10 days and is characterized by a distended uterus and enlarged abdomen.
In more severe cases, the amount of fluid may reach 80-120 litres, thus, the weights of fluid, membranes and uterus frequently total 350-550 pounds.
The excessive volume of fluid distending the abdomen causes the owner to believe that of breeding dates are wrong or else the cow is going to have triplets.
Digestive symptoms with anorexia, lack of ruminations and constipation are noted.
The cow may drink excessive water. The pulse is elevated to 90 to 140 per minute and is weak and wiry.
The cow may exhibit anxiety, restlessness and an expiratory grunt.
As the condition progresses, the abdomen becomes more distended. The gait is stiff, slow and cautions. The cow loses body condition and eventually is unable to rise. Dislocation of the hips or backward extension of the rear limbs may occur and the cow lies on her sternum looking like a “bloated bull frog”.
Rarely rupture of the prepubic tendon or ventral hernia may occur due to the excessive weight of the uterus.
Rectal examination
- Uterus is distended and tense.
- Placentomes can seldom be felt due to the tense uterine wall but the uterine arteries are whirring indicative of a live fetus.
- The uterus appears to fill the abdominal cavity.
Differential diagnosis
- Indigestion
- Bloat
- Traumatic gastritis
- Hydramnios
Prognosis
Prognosis of hydrallantois is poor. In advanced cases in which the cow is unable to rise, the prognosis is often hoepeless. Even if the fetus can be removed the mortality of the cow may occur because the uterus is atonic, the membranes are diseased and shock or severe septic metritis usually follows hydrallantois.
Even if the cow survives its reproductive life is questionable. Retained placenta and septic metritis are common sequelae in hydrallantois.
Treatment
Varies with the duration and severity of the condition.
In mild cases: undiagnosed until abortion / premature birth / parturition, excessive volume of fluids are observed accompanied by the presence of a poorly viable or dead fetus. Mutation and forced extraction of these foetuses are usually easily effected.
Retained placenta and septic metritis usually follows hydrallantois. Early treatment for these conditions with parentral and local antibiotics and ecbolics such as oxytocin, stilboestrol and ergonovine are indicated.
In severe cases with a closed cervix, the prompt termination of the abnormal pregnancy is desired. The parturition is induced with corticosteroids or PGF2α or both. Assistance and lubrication at the time of delivery is essential.
Caesarean section is performed as a last resort. Fluid therapy and proper post-operative care is essential. Following caesarean section, refilling of the uterus also noticed. It requires further drainage.
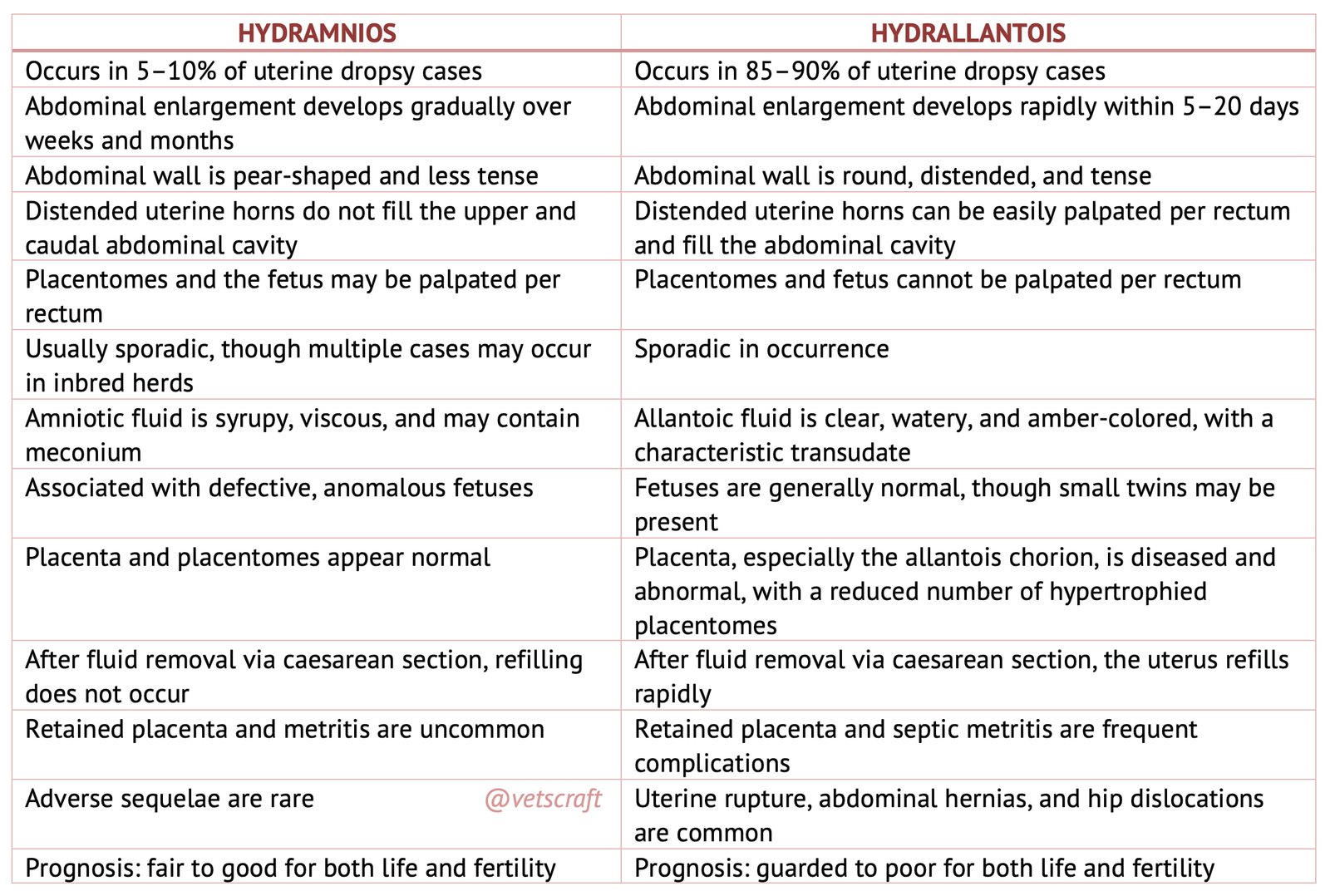
Differences between Hydramnios and hydrallantois