TABLE OF CONTENTS
Examination of an Obstetrical Case
The examination of an obstetrical case in animals requires a systematic and careful evaluation to ensure the safety of both the dam and the fetus.
Before proceeding to interfere with the animal, a comprehensive history of the case should be obtained.

Much of it will be the outcome of questioning the attendant, but many points will also be elicited from personal observation of the animal.
- Is the animal primiparous or pluriparous?
- Has full term arrived, or is the delivery premature?
- Is the animal a primigravida or multigravida?
- What is her previous breeding history?
- When did straining begin, and what was its nature—slight and intermittent or frequent and forceful?
- Has straining ceased?
- Has a water bag appeared, and if so, when was it first seen?
- Has there been any escape of fluid?
- Have any parts of the fetus appeared at the vulva?
- Has an examination been made, and has assistance been attempted? If so, what was its nature?
- In the case of multiparous species, have any young been born—naturally or otherwise—and if so, when? Were they alive at birth?
- Is the animal still taking food?
- Is the animal able to get up if recumbent?
By considering the answers to these and similar questions, it is possible to form a fairly accurate idea of the case.
General Examination of the Animal
Assess the physical condition—whether the animal is thin and emaciated, too fat, or in good condition.
If the animal is recumbent, determine whether it is able to rise or is exhausted.
Body temperature and pulse rate should be noted, and the significance of any abnormalities considered.
Particular attention should be paid to the vulva. Parts of the fetus may be protruding, and it may be possible to assess the nature of the dystocia from these. Are any exposed fetal parts moist or dry? Such evidence not only serves as a guide to the duration of the condition but also to the effort that will be necessary to correct it.
Should parts of the amnion protrude, what is their condition? Are they moist and glistening, and is fluid caught up in their folds? If so, their exposure is recent and the case is an early one.
If the membranes are dry and dark in colour, it may be taken that the case is delayed.
Particular attention should be paid to the nature of the discharge.
Blood, especially if profuse, indicates recent injury to the birth canal.
A dark brown, fetid discharge indicates a grossly delayed case.
In dystocia of the bitch, the onset of vomiting together with a great increase in thirst should be regarded as grave signs.
Special Examination and Restraint
The specific examination, consisting of a detailed examination of the genital tract and fetus, should be undertaken only after the animal has been properly confined and restrained.
A well-ventilated area with good lighting and easy access to hot water is essential for obstetrical operations.
In nearly all cases of dystocia, a standing position or the elevation of the rear parts is necessary to allow the veterinarian to work with relative ease and to effect a prompt correction of the dystocia.
The animal’s external genitalia and surrounding structures should be thoroughly washed with warm water and soap. In sheep and long-haired dogs, it is necessary to clip the hair in the perineal area. In the mare, the tail should be bandaged.
In cattle, epidural anaesthesia is helpful in preventing frequent defecation during obstetrical operations. In some cases, however, epidural anaesthesia might not be desirable, as it causes cessation of straining—this straining may be helpful in the withdrawal of a normally presented fetus.
The birth canal should be examined to determine whether it is dilated, twisted, moist or slippery, inflamed, swollen, dry, necrotic, contains pathological bands, has stenotic areas, or contains gummy mucus—indicating that parturition has not yet begun or is in its early stages.
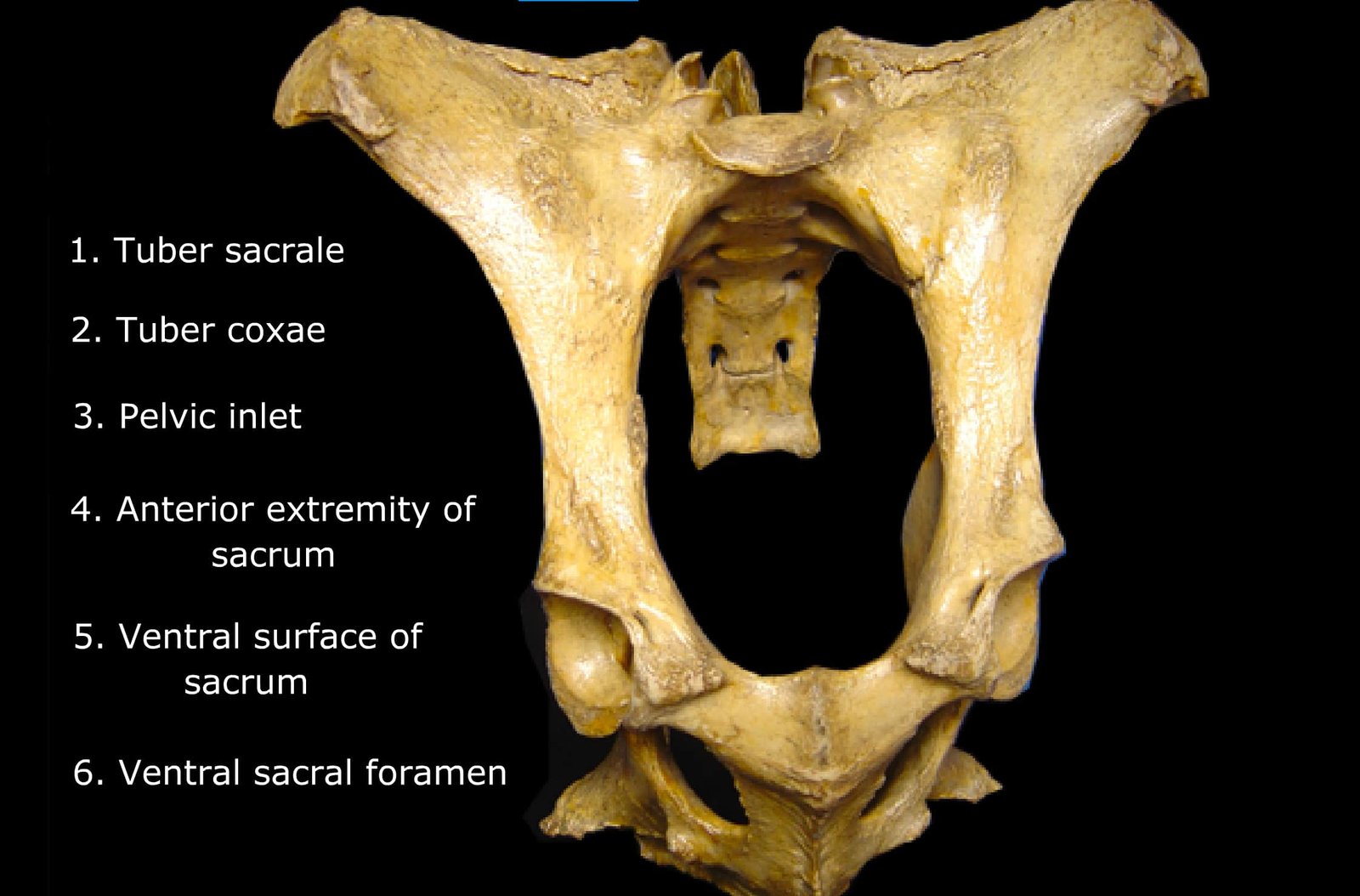
The degree of dilation or relaxation of the cervix should be noted, as well as any evidence of torsion. The size of the pelvic inlet, vulva, and vagina in relation to the size of the fetus should be assessed.
The fetus should be examined to determine whether it is dead or alive, as this will influence the prognosis and affect the management of the case.
If the fetus is alive:
- Grasping the foot and pulling it may cause movement of the limb (pedal reflex).
- Pinching the eyeballs may cause the fetus to shake its head (corneal reflex).
- Placing fingers in the fetus’s mouth may induce suckling or tongue/jaw movements (suckling reflex).
- In a posterior presentation, inserting fingers into the anus may cause contraction of the anal sphincter (anal reflex).
If the fetus is dead, the degree of decomposition should be accurately assessed by evaluating subcutaneous edema or emphysema, sloughing of fetal hair, and putrid, fetid odour.
The fetus should be carefully examined for any abnormalities in presentation, position, posture, or teratologic defects.
In breech presentation, the tail is often observed hanging from the vulva or lying in the birth canal.
If feet are lying in the birth canal, it should be determined whether they are front or hind limbs:
- Front limbs have two joints—fetlock and knee—between the hoof and elbow.
- Hind limbs have only one joint between the hoof and hock.
If feet are protruding through the vulva with the soles ventral (facing the ground), the fetus is likely in either anterior longitudinal, dorsosacral position or posterior longitudinal, dorso-pubic position.
If the soles are dorsal (facing upward), the fetus is in either posterior longitudinal, dorsosacral position or anterior longitudinal, dorso-pubic position.
If more than two limbs are entering or near the pelvis, the condition should be carefully evaluated to differentiate between:
- Twins wedged in the pelvis
- A schistosomus reflexus
- A double monster
- In the mare, a transverse ventral presentation
It may occasionally be necessary to repel the fetus out of the birth canal and into the uterus to accurately diagnose the cause of the dystocia.