TABLE OF CONTENTS
Antiarrhythmic drugs
Synonym of Antiarrhythmic: Anti-Arrhythmia / Anti-Dysrhythmia
Antiarrhythmic drugs are agents used to control ectopic foci or reverse disorganised conduction of electrical impulses through the heart. Although research has provided some information regarding the cellular mechanisms of arrhythmias and the mode of action of antiarrhythmic drugs, the general approach to therapy remains empirical.
Read “Arrhythmia and it’s types“
Classification of antiarrhythmic drugs
Antiarrhythmics or antidysrhythmic are classified as follows-
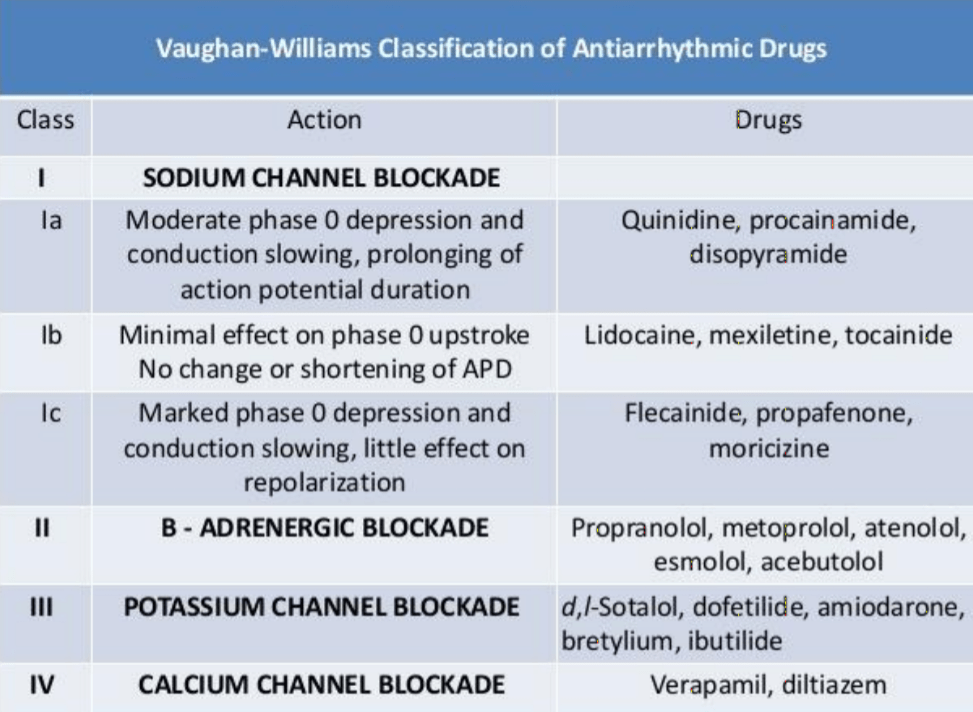
- Class I – drugs act by blocking the sodium channel– They are subdivided into 3 subgroups, IA, IB, and IC, based effects on phase-0 deploarization and repolarization:
- Subclass IA drugs have moderate potency at blocking the sodium channel and also usually prolong repolarization (increase QRS) Eg. quinidne, procainamide, disopyramide
- Subclass IB drugs have the lowest potency as sodium channel blockers, produce little if any change in action potential duration, and usually shorten repolarization. Eg. lidocaine (Lignocaine), phenytoin
- Subclass IC drugs are the most potent sodium channel blocking agents, and have little effect on repolarization (increase PR, increase QRS) Eg. flecainide, encainide
- Class II drugs act indirectly on electrophysiological parameters by blocking beta-adrenergic receptors (increasing PR)– Example is propranolol.
- Class III drugs act by mechanisms that are not well understood (interference with potassium conductance is one possible mechanism), but act to prolong repolarization (increase refractoriness), with little effect on the rate of depolarization (QT). eg. sotalol, amiodarone
- Class IV drugs act by blocking the voltage-sensitive calcium channels– They slow the conduction in the S-A and A-V nodes where action potential propagation depends on slow inward calcium current. eg. verapamil, nifedipine.
- In addition to the above classes, there is also a miscellaneous group of drugs that includes digoxin, adenosine, and alinidine (a chloride channel blocker):
- Drugs within a class are not necessarily clinically similar: a patient may respond well to one drug in a given class, but not another.
- Almost all of the currently available drugs have multiple actions; in agiven patient, it is difficult to establish which action is responsible for the action
- The metabolites of some drugs contribute to or are primarily responsible for their antiarrhythmic actions (e.g.- procainamide and its metabolite, N-acetylprocainamide; encainide and its metabolite, 3-methoxy-O-desmethylencainide).
