TABLE OF CONTENTS
Traumatic Reticulo Peritonitis (TRP)
Traumatic Reticulo Peritonitis (TRP) and allied disorders are also known as Hardware Diseases because they are caused by nails, parts of tense wire, and metallic substances.
Allied disorders are vagus indigestion (due to damage to the vagus nerve), diaphragmatic hernia, and aberrant injury to other vital organs. Also called as Hardware disease because 90% of conditions are due to the ingestion of metallic foreign bodies. TRP is a common field condition encountered in bovines that is clinically characterised by the sudden onset of anorexia, decreased milk yield in lactating animals, Recurrent Tympani, ruminal stasis, and associated signs of abdominal pain.
If Traumatic Reticulo Peritonitis (TRP)’s foreign body pierces the pericardial sac, it causes Traumatic Pericarditis.
Etiology
The majority of the cases are caused by the ingestion of metallic foreign bodies, and the animals (bovines) are indiscriminately fed.
Pathogenesis
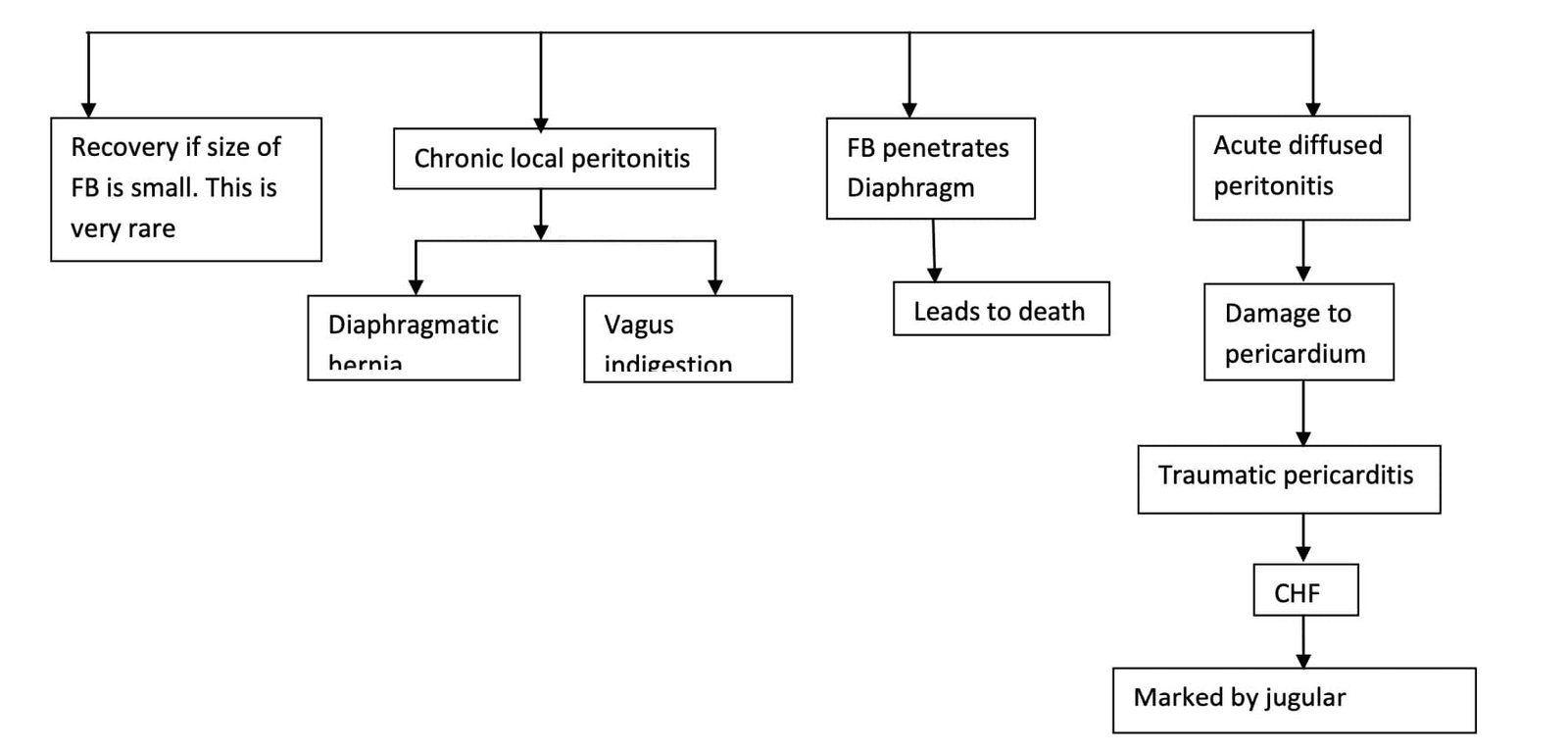
The ingested foreign body goes to the rumen. 1st to the dorsal sac, then to the ventral sac, and then, by ruminal contraction, it gets passed into the reticulum. The mucosa of the reticulum has a honeycomb structure, so it gets trapped in the reticulum (cranio-ventral location), which causes traumatic reticullitis. Thereafter, the foreign body keeps on piercing through the reticulum wall, resulting in local peritonitis due to spillage of reticular contents. Initially, it is acute, and if the foreign body gets adhered to, it results in chronic peritonitis. The extensive spread of infection in the peritoneal cavity causes diffused peritonitis, which is always acute and responsible for deaths in the majority of cases.
Sequalle of ingested foreign body
Uncommon sequelae
- Rupture of the left gastro-epiploic artery causes massive internal haemorrhage, leading to instantaneous death.
- Traumatic spleenitis, spleenic abscess, diaphragmatic abscess. If the foreign body (FB) is small, the lower anterior part of the reticulum is the most common route of escape for the foreign body out of the rumen.
- Aberrant passage of FB into the thoracic cavity can cause lung abscesses, traumatic peritonitis, and mediastinal abscesses.
- Right axial abscess (right elbow): here, FB, due to the presence of rumen and reticulum on the left side, passes on the right side and gets fixed in the right intercoastal muscle, leading to abscess formation.
- If FB is very sharp, it results in heart rupture and haemorrhage called cardiac tempanode, leading to cardiac arrest and death.
Clinical findings
- Acute local peritonitis: Onset is quite sudden, complete anorexia, sharp decrease in milk yield, animal shows signs of abdominal pain-kicking at belly, reluctant to move, cautious gait. This is accompanied by a grunt. This sign is more prominent when an animal is walking down a slope; due to gravity, there will be pressure on the foreign body by the abdominal organs.
- Appearance: Tucked-up appearance (kyphosis); dorsal curvature (arched back). All this indicates some abnormality in the xephoid region. The signs of pain and grunts are much more pronounced during urination and defecation.
- Systemic reaction: Moderate fever (103 to 104 °F), high pulse rate, respiratory rate increased (due to ongoing toxaemia). Usually, ruminal contractions are decreased with suspended rumination, and there is always the presence of moderate tympani, which is called recurrent tympani. Usually there is constipation and passage of dry hard faeces (due to decreased intestinal motility because of peritonitis and toxaemia-ingesta remains for a longer period and there is increased water absorption leading to dry hard faeces).
- Pain: Deep palpation with fist behind xiphoid cartilage-animal immediately shows grunt. This is called the Fist test. In chronic local peritonitis, the signs develop gradually.
- Diffused peritonitis: Always acute, Onset is sudden with prolonged toxaemia, and there is severe depression. If the case is presented early, the temperature is usually high, but later it is subnormal. Most of the time, the animal is in a recumbent state, indicating a terminal stage, and at this stage, if treatment is not initiated, the animal enters a state of coma and death. But in the terminal stage, when the animal is in lateral recumbency, bradycardia with arrhythmia is noticed, along with a highly congested cyanotic membrane.
Diagnosis
The diagnosis of Traumatic Reticulo Peritonitis (TRP) can be made based on the animal’s history and clinical signs. Another diagnostic that can be used is:
Clinical examination of animal
- Appearance/Posture: Tucked-up appearance and winged elbow
- Physical examination: bamboo test or Ploe test, in which a thick wooden pole is passed behind the elbow and the animal is lifted. If an animal makes a loud grunt, it indicates pain in the xiphoid.
- Either pinch or spinal pinch: Here, because of the wither pinch, the animal makes a lardosis posture with a loud grunting sound. If the grunt is mild, then it can be heard by keeping the diaphragm of the stethoscope on the chest or trachea.
- Williams’s method of simultaneous palpation and auscultation (At 7-9th intercostal space): the reticulum approximates the diaphragm. The chest piece of the stethoscope is kept, and by right hand, the first rumen is palpated or pushed. By doing so, some of the ruminal contents are moved to the reticulum, which can be heard as a reticular splashing sound. If this is a grunt, it is an indication of TRP.
Laboratory investigation
- TLC and DLC help differentiate between types of peritonitis. The typical picture of acute peritonitis is neutrophilia with a shift to the left. This is considered a negative shift to the left since the number of band cells does not exceed the mature neutrophil count.
- Peritoneal fluid analysis: Peritoneal fluid is collected by abdominal paracentesis at 10 cm cranial and 10 cm to the right side of the umbilicus. In adult cattle, the tip of the needle should not be too sharp to avoid injury to visceral organs. 10–20 ml of fluid is collected and examined for Nucleated cell count, Protein estimation and Fibrinogen level.
Ferroscopy
Magnets and metal detectors—to and fro movements are made at Xiphoid region.
Radiographic investigation
500 mA x-ray machine is required for large animals. It not only helps in indicating metallic FB but also helps in identifying its location and the integrity of the diaphragmatic line.
Laparoscopy
Right flank laparoscopy with a semi-rigid fibre optic laparoscope is also proving to be a reliable diagnostic method.
Exploratory laparotomy
An exploratory laparotomy can be performed to search for a foreign body in a suspected case of Traumatic Reticulo Peritonitis (TRP).
Differential diagnosis
- Bovine pyelonephritis: Signs of abdominal pain are seen, but this is accompanied by pus or blood in the urine.
- Abdominal displacement: Here also ruminal stasis, passing pasty faeces, and prolonged inappetance are indicative, but recurrent tympani, cautious walking, and kyphosis are absent. The ballooning structure in the mid flank region is seen in displaced abomasums. Here, faeces are scanty and pasty, but in TRP, faeces are hard and mucous-coated.
- Ephemeral fever: The illness lasts only 3 days; shifting lameness; lymph node enlargement; and seasonal occurrences are common.
Treatment
Conservative medical therapy:
This is done when surgery can’t be taken due to the debility of the animal or an advanced pregnancy. The first priority here is immobilisation of the animal. This is done by confining the animal in a box-stall with a minimum space for movement, immobilisation facilities, and the formation of adhesions, which restricts further passage of FB.
Surgical approach (Rumenotomy)
Rumenotomy is usually done on the left flank:
- If adhesions are there, they are removed to avoid complications like vagus indigestion.
- The presence of FB is checked.
- The extension of peritonitis is arrested.
- Then rumenotomy is advocated. 2/3rd contents are removed, and then the reticulum is searched for FB.
- Recovery depends on the time of surgery and complications.
- Failure of improvement is due to diffused peritonitis, escape of FB beyond the diaphragm, and involvement of other organs.
Prevention and Control
- Chaffed feed should be passed over a magnetic field or belt to trap metallic objects.
- Feeding of magnets with cylindrical or bars with rounded edges. (Size: 7.5 long, which can be retrieved periodically.)

