TABLE OF CONTENTS
Chronic Luxation of Patella in Cattle
Chronic Luxation of Patella in Cattle is the impaired patellar function characterized by jerky movements during flexion to complete immobilisation of the joints.
Animal fixes its ‘limb in extension’ while the patella glides up over the trochlea to its maximum height on the articular surface.
Chronic Luxation of Patella in Cattle may be recurrent or permanent upward fixation of the patella could be seen. It is more common in draught purpose animals.
It is non-inflammatory functional disorders of the femoro-patellar articulation in cattle.
When one limb involved, animal moved forward by swinging the rigid affected limb outward and forward.
Some Points on ‘Patella‘
Patella is a large sesamoid bone. It is connected to femur by collateral ligaments and to the cranial tibial tuberosity by patellar ligaments. Patellar ligaments are medial, middle and lateral.
Laxity of the patellar ligaments predisposed the animal to upward fixation of the patella. Relaxed ligaments allow the patella to glide freely on the articular surface of the trochlea.
If limb is over extended, the patellar apex may get jammed between the trochlear ridges by hooking the medial fibrocartilage over the medial trochlear ridge. cutting the medial patellar ligament solve the fixation and animal recovers.
Etiology of Chronic Luxation of Patella
- Major potential factors for patellar fixation in cattle are “nutrition deficiency”
- External traumas
- Breed and genetic predisposition Morphological changes of the medial trochlea ridge of the femur
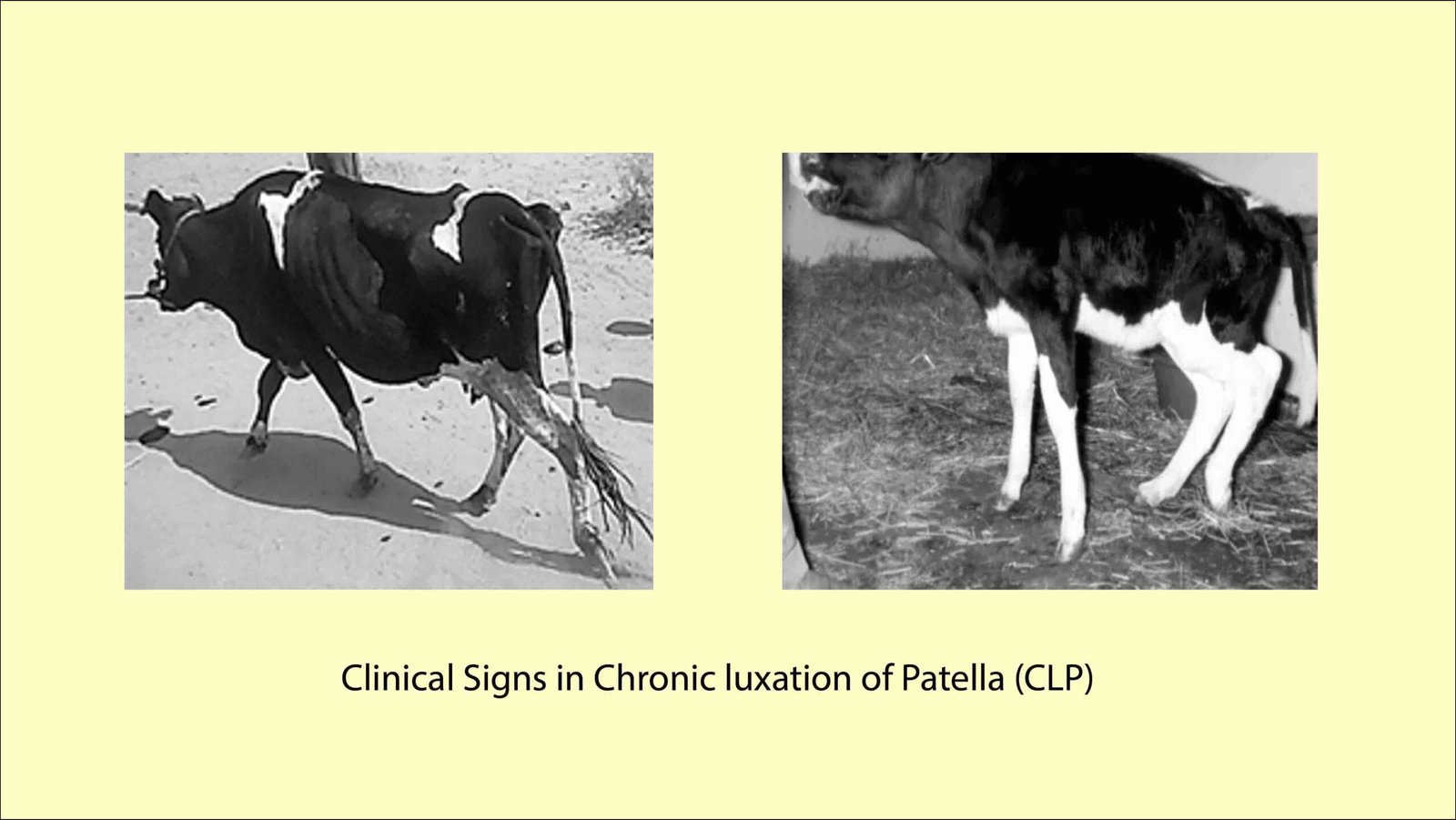
Clinical Signs of Chronic Luxation of Patella
- Posture of the animal is normal at rest but, every attempt to move the animal backwards is resisted.
- Animal shows jerky flexion during movements or drags the affected limbs with flexed pastern.
- Affected limb is brought forward with a jerky flexion on every step.
- While sitting – affected limb stretched
Objective
The patella gets fixed above the trochlea of femur and the medial straight ligament is tightly overstretched behind the medial trochlear ridge, which prevents the downward return of the patella.
The objective of the operation is to mechanically bring down the patella by cutting the tensed medial ligament.
Treatment of Chronic Luxation of Patella
The subcutaneous division of the medial patellar ligament is the common surgical treatment to correct upward fixation of the patella-
- Bassi’s method – In western countries
- Open method
- Stab or Closed method
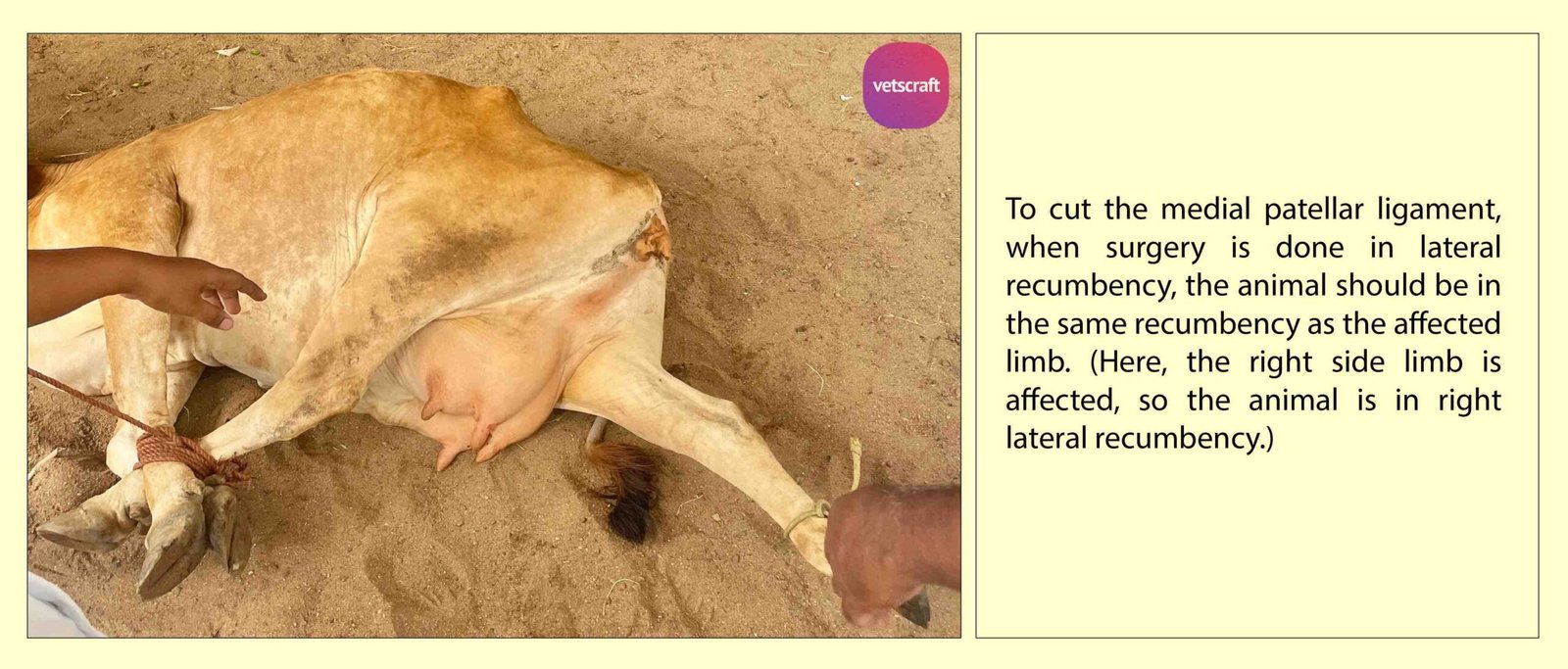
Clinicians prefer the surgery in the standing animal, in lactating animal a lateral recumbency is preferred.
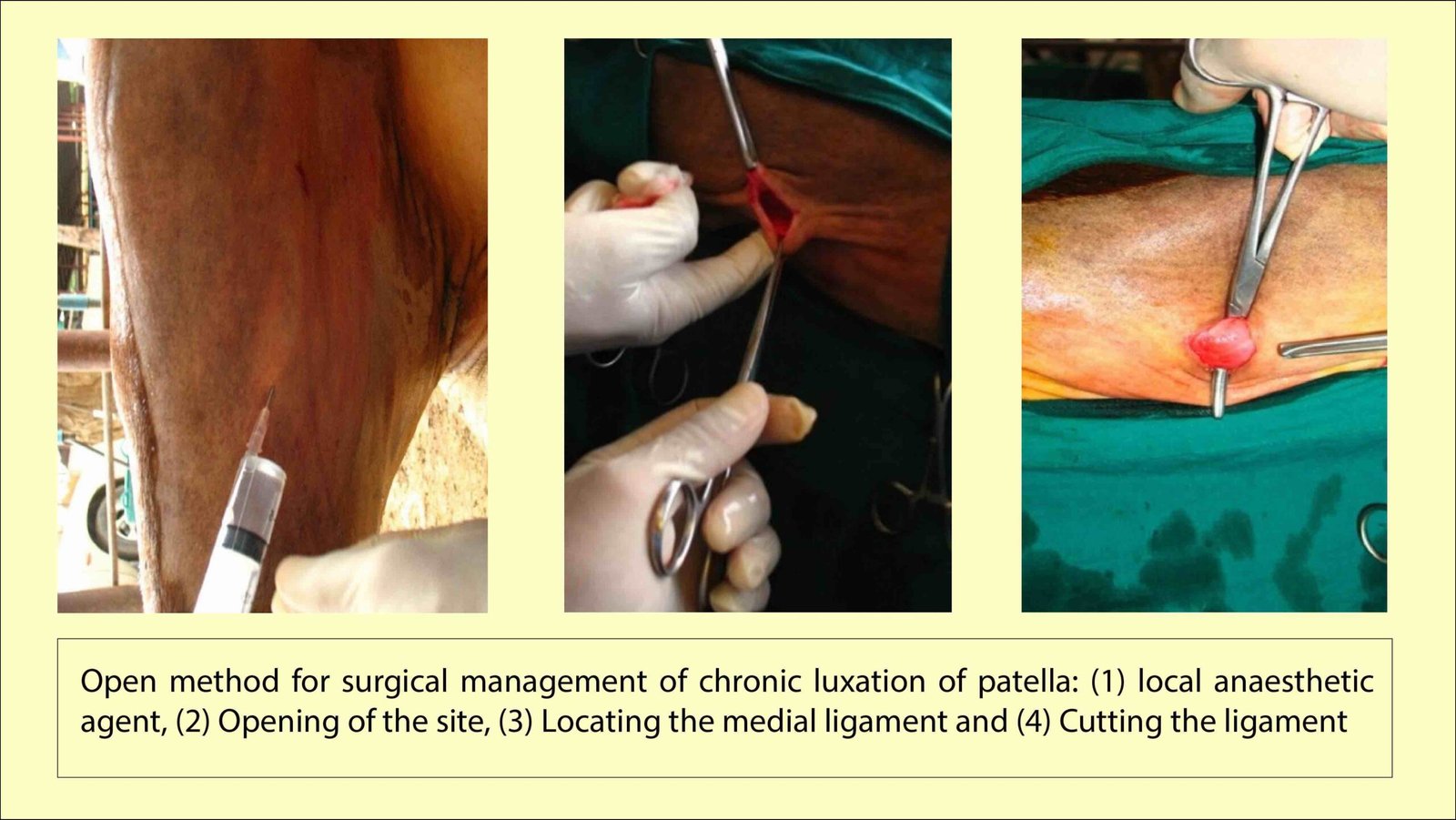
The site is prepared for aseptic surgery and infiltrated with local anaesthetic solution (2% Lignocaine, 2-5ml).
Locating Medial Patellar Ligament
- The index finger is moved upward along the cranial border of the tibia till the cranial tibial tuberosity is reached.
- The cranial ligament is traced as a broadest and thickest among the three patellar ligaments.
- The finger is then moved over the medial ligament which is felt as a prominent cord.
Open Method
A small incision is made in the skin directly over the medial ligament. The index finger is passed into the wound and the skin separated from the fascia all around the site.
The fascia is dissected to expose white glistening medial patellar ligament. the ligament is exteriorized by passing a curved scissors.
The ligament is then sectioned near its insertion using a knife. the cutaneous wound is sutured with one or two interrupted sutures which are removed on seventh or eighth postoperative day.
Cessation of crunching sound and immediate relief of the characteristic jerky flexions during progression are indications of a successful medial patellar desmotomy.
Closed Method
A stab incision is made into the skin with a B.P. Blade immediately in front of the medial tibial tuberosity.
Through this incision, the abscess knife, curved probe pointed knife or hey groove knife or tenotomy knife is passed flat wise between the middle and medial patellar ligaments and the sharp edge of the instrument is directed towards the ligaments.
The ligament is then transected by withdrawing the knife towards the operator.
A small quantity of tincture iodine is instilled into the wound which is left unsutured.
A piece of the ligaments is removed to prevent the reunion of cut ends of the ligaments.
Cessation of crunching sound and immediate relief of the characteristic jerky flexions during progression are indications of a successful medial patellar desmotomy.